
English
CALIFORNIA
DRIVER’S HANDBOOK
This handbook is available at
dmv.ca.gov
Gavin Newsom, Governor
State of California
Toks Omishakin, Secretary
California State Transportation Agency
Steve Gordon, Director
California Department of Motor Vehicles

• Renew driver’s license
and vehicle registration
• Replace sticker or registration
• Change address
• Request driver’s record
• Request vehicle record
• And more
…
We know your time is
valuable

i
Dear fellow Californian,
Whether traveling by car, transit, bike, scooter,
skateboard or on foot, we all want to reach our
destination safely. Tragically, many Californians do
not.
Since 2010, more than 30,000 people have been
killed and another 100,000 people seriously
injured on California roads. This deadly trend
is getting worse, especially for people walking or biking. We’ve seen
a nearly 50 percent rise in annual deaths and serious injuries for
pedestrians and greater than 60 percent increase in bicyclists killed per
year since 2010.
Unlike those of us traveling in vehicles with seat belts, airbags and other
safety features, people outside of vehicles don’t have the same level
of protection and are more vulnerable every time they are on the road.
Their safety must always be top of mind when we’re driving.
California is doing everything possible to implement comprehensive
traffic safety measures to eliminate deaths and serious injuries on our
roadways. It includes strategies to reduce our dependence on driving,
to the way we design roads and intersections, to expanding safe walking
and biking options.
But we need your help. Without all of us practicing safe driving habits,
these avoidable tragedies will continue to occur. Please make sure to
buckle up, follow all traffic laws, pay extra attention to pedestrians and
bicyclists, and do not drive if you’re distracted or impaired.
I hope the information in this California Driver’s Handbook can help
everyone on the road – drivers, bicyclists and pedestrians – reach their
destination safely. Because it’s about more than just learning the rules of
the roads. It could be a matter of life and death.
Wishing you safe journeys,
Toks Omishakin
Secretary
California State Transportation Agency

ii
C
© Copyright, Department of Motor Vehicles 2024
All rights reserved.
This work is protected by U.S. Copyright Law. The Department of Motor
Vehicles (DMV) owns the copyright to this work. Copyright Law makes it
illegal to:
1. Make a copy of any part of this handbook.
2. Print copies of this handbook and give them to other people.
3. Write your own version of this handbook.
4. Put this handbook on public display.
5. Perform (read aloud) the handbook in public.
If you have questions about whether you can make copies of any part of
this handbook, address them to:
Department of Motor Vehicles
Legal Office, MS C128
PO Box 932382
Sacramento, CA 94232-3820
Disclaimer
This handbook is a summary of the laws and regulations in the Vehicle
Code available at leginfo.legislature.ca.gov. DMV, law enforcement, and
the courts follow the full, exact language.
Contact Us
Send comments or suggestions for this driver’s handbook to
dmv.ca.gov/customerservice.

iii
T C
SECTION 1. The California Driver’s License ......................................................1
SECTION 2. Getting an Instruction Permit and Driver’s
License .......................................................................................................................2
SECTION 3.
The Testing Process ............................................................................ 5
SECTION 4. Changing, Replacing, and Renewing Your
Driver’s License ...................................................................................... 8
SECTION 5. An Introduction to Driving ............................................................. 9
SECTION 6. Navigating the Roads ...................................................................... 13
SECTION 7. Laws and Rules of the Road ...................................................... 33
SECTION 8. Safe Driving ...............................................................................................57
SECTION 9. Alcohol and Drugs...............................................................................72
SECTION 10. Financial Responsibility, Insurance
Requirements, and Collisions .................................................. 76
SECTION 11. Vehicle Registration Requirements ................................... 79
SECTION 12. Driver Safety ..........................................................................................80
SECTION 13. Seniors and Driving ......................................................................... 82
SECTION 14. Glossary ....................................................................................................84

iv
DMV S
Have your driver’s license or identication (ID) card number, vehicle
license plate number, or vehicle identication number (VIN) available.
Online Services
Vehicle Registration Renewal at dmv.ca.gov/vrservices.
Driver’s License Renewal at dmv.ca.gov/dlservices.
Office Appointments at dmv.ca.gov/make-an-appointment.
Visit dmv.ca.gov/online to nd many other online services.
Kiosk Services
Visit dmv.ca.gov/kiosks to nd kiosk services and locations.
Phone Services
Call 1-800-777-0133.
During Normal Business Hours:
• Talk to a DMV representative.
Automated 24/7 Phone Services:
• Renew your vehicle registration.
• Make a DMV office appointment.
Individuals who are deaf, hard of hearing, or speech impaired may call
1-800-368-4327 for assistance.

1
SECTION 1. The California Driver’s License
A California driver’s license allows you to drive on public roads.
Before you can get a driver’s license in California, you are required
to pass the knowledge and behind-the-wheel drive tests based on
information in this handbook.
You must have the correct license to drive your vehicle type. Most
people need a noncommercial Class C driver’s license. To operate
commercial vehicles, motorcycles, and other types of vehicles, you
must have a different class of license.
For information on vehicles covered by a Class C, visit dmv.ca.gov/dl.
C D
REAL ID Driver’s License
Beginning May 2025, your driver’s license or identication (ID) card must
be REAL ID compliant if you use it to:
• Board an airplane for domestic ights.
• Enter military bases.
• Enter most federal facilities.
Visit dmv.ca.gov/realid to learn more about applying for a REAL ID.
Driver’s Licenses for Undocumented Residents
California offers driver’s licenses for all residents regardless of
immigration status. For more information, visit dmv.ca.gov/dl.
Organ and Tissue Donor
For information, visit donateLIFEcalifornia.org.
Veterans
Visit dmv.ca.gov/veterans to learn more about the requirements and
benets of a Veteran designation.
ID Cards
ID cards are issued for identication purposes to eligible persons of any
age. They do not permit you to drive. To get an ID, you must provide your
identity document, residency documents, and social security number.
Visit dmv.ca.gov/id-cards to complete an ID card application and get
information on current acceptable documents and reduced-fee, no-fee,
or senior ID cards.

2
SECTION 2. Getting an Instruction Permit and
Driver’s License
If you do not have a driver’s license from California or another state, you
must apply for an instruction permit before taking the behind-the-wheel
drive test to get your driver’s license.
W Y N
To apply for an instruction permit or driver’s license, you must provide:
• Proof of identity: Proving who you are.
• Two proofs of residency: Proving you live in California. Exceptions
may apply.
• Legal full name document: Proving your current name if the name
on your identity document and application do not match.
• Social security number: Exceptions may apply.
For REAL ID requirements, current acceptable documents, and eligibility,
visit dmv.ca.gov/realid.
R T V
For information on registering to vote, visit California Secretary of State at
sos.ca.gov.
A F A I P
To apply for a Class C instruction permit:
1. Complete a Driver’s License & ID Card Application.
2. Provide your documents.
3. Pay a non-refundable application fee.
4. Pass your knowledge test(s).
5. Pass a vision test.
For more information, visit dmv.ca.gov/instructionpermit for a complete
list of application steps and requirements.

3
If you are under 18 years old, you will also need to:
• Be at least 15½ years old.
• Complete a driver education program.
• Have a parent or guardian sign to approve the application and accept
nancial responsibility (see Section 10). If your parents or guardians
share joint custody of you, both must sign.
• Wait to use your instruction permit until you start behind-the-wheel
driver training with an instructor who will validate the permit.
D S
Driver education and driver training are offered at DMV-licensed driving
schools and some high schools. Instructors must carry an instructor’s ID
card. Ask to see it.
See the Driver Training Schools page at dmv.ca.gov/driver-ed for more
information about selecting a driving school.
A F A D’ L
To get your driver’s license after you have your instruction permit,
you need to:
• Practice driving with a California-licensed driver who is at least 18
years old (25 for minors). This person must sit close enough to take
control of the vehicle if needed.
• Pass a behind-the-wheel drive test.
If you are under 18 years old, you will also need to:
• Be at least 16 years old.
• Have an instruction permit from California or another state for at least
6 months (or turn 18 years old) before scheduling your behind-the-
wheel drive test.
• Prove that you completed both driver education and driver training.
• Practice driving for at least 50 hours with a California-licensed driver
who is at least 25 years old. Ten hours must be at night.
See the Driver’s Licenses page at dmv.ca.gov/dlservices for the
complete list of application steps, requirements, the Parent Teen Driving
Contract, and Driving Performance Evaluation (DPE) Score Sheet.

4
Minor’s Restrictions and Exceptions
When you are under 18 years old, your driver’s license will have the word
provisional. As a provisional driver, you cannot drive:
• Between 11 p.m. and 5 a.m. during the rst 12 months you have your
license.
• With passengers under 20 years old, unless your parent or guardian
or other California-licensed driver (at least 25 years old) rides with
you.
• For pay or operate vehicles that require a commercial Class A, B, or C
license.
There are exceptions to these restrictions if you:
• Have a medical need and cannot reasonably nd another way to
travel. You must carry a note signed by your physician. The note must
have your medical condition and date you are expected to recover.
• Drive for schooling or a school activity. You must carry a note signed
by your school principal, dean, or designee.
• Must drive for work reasons. You must carry a note signed by your
employer. The note must conrm your employment.
• Must drive an immediate family member. You must carry a note
signed by your parent or legal guardian. The note must state the
reason you need to drive, the family member, and date when the
need will end.
NOTE A parent or guardian may cancel their teen’s license by
completing a Request for Cancellation or Surrender of a Driver License
or ID Card form.

5
SECTION 3. The Testing Process
D’ L T
Here is an overview of the driver’s license tests:
1. Vision Test
DMV tests all applicants to ensure they can see well enough to drive
safely. If you take your vision test with corrective or contact lenses,
your driver’s license will have a corrective lenses restriction. If you do
not pass your vision test, you will be asked to have your eye doctor
complete a Report of Vision Examination form. For more information, visit
dmv.ca.gov/vision-standards.
2. Knowledge Test
When you apply for an original driver’s license, you must pass a
knowledge test with multiple choice questions. You are allowed three
attempts to pass before you must reapply. Minors must wait seven days
to retake a failed knowledge test, not including the day of the failure.
Testing options will be available once you complete your application at
dmv.ca.gov/dl.
IMPORTANT: You are not allowed to use any testing aids during
knowledge tests, such as a California Driver’s Handbook or cell phone.
3. Behind-the-Wheel Drive Test
When you apply for an original driver’s license, you will be tested on your
ability to safely drive a vehicle. Upon renewal, drivers with a vision or
medical condition may be required to take a behind-the-wheel test. The
examiner may give two or more instructions at one time to determine
whether you can understand and properly follow both directions.
For example, “At the next street, make a left turn, and then at the rst
intersection make another left turn.”
Visit dmv.ca.gov/make-an-appointment to schedule a behind-the-
wheel drive test appointment.

6
On the day of your behind-the-wheel test, you must bring:
1. Your instruction permit or driver’s license (if you have one).
2. Another California-licensed driver who is at least 18 years old (25 for
minors), unless you are already licensed to drive.
3. A vehicle that is safe to drive for your test.
4. Valid proof of insurance and vehicle registration.
5. If you plan to use a rental vehicle for your drive test, your name must
be listed on the rental contract. The contract must not exclude
behind-the-wheel drive tests.
NOTE Minors must wait 14 days to retake a failed behind-the-wheel
drive test, not including the day of the failure.
Before you begin, the DMV examiner will ask you to locate and
demonstrate the following:
• Driver window – The window on the driver side must open.
• Windshield – The windshield must allow a full, clear, unblocked view
for you and the DMV examiner. Windshield cracks may postpone your
test.
• Rearview mirrors – At least two rearview mirrors. One of them must
be on the left side of your vehicle.
• Brake lights – The right and left brake lights must be operational.
• Tires – The tires must have at least 1/32-inch of uniformed tread
depth. The use of a donut tire is not allowed during a drive test.
• Foot brake – There must be at least one inch of clearance between
the bottom of the brake pedal and the oorboard when depressed.
• Horn – Designed for the vehicle, in proper working condition, and
loud enough to be heard from a distance of at least 200 feet.
• Emergency (parking brake) – How to set and release the parking
brake.
• Turn/Arm signals
a. Left turn.
b. Right turn.
c. Slowing down or stopping.
• Windshield wipers: control arm or switch – You may be required to
show they function.
• Seat belts – All seat belts must work properly and be used by the
individual(s) in the vehicle.
NOTE If your vehicle does not meet the requirements, your drive test
will be rescheduled.

7
Interpreters may be used during the pre-drive inspection for the
identication and use of certain controls in the vehicle but may not
accompany you during the drive test.
Only the examiner is allowed to accompany you during the drive test.
Exceptions are made for training, service animals, and certain law
enforcement situations.
The use of a recording device, including a video recorder, is prohibited
during a behind-the-wheel drive test. If the recording device cannot be
powered off or disabled, the applicant must block it so there is no visual
or audio recording during the drive test.
Other Things to Know for Your Behind-the-Wheel Test
The drive test is intended to determine your skill in operating a motor
vehicle in most road situations and evaluate your abilities, not the
vehicle’s technology. Therefore, advanced driver assistance systems
technologies, such as automated parallel parking, lane departure, and
adaptive cruise control, are not permitted during the drive test. Vehicle
safety technology, such as backup cameras and blind spot monitors, may
be used on the drive test, but are not a replacement for an actual visual
check of your mirrors and blind spots.
To view a sample of the Driving Performance Evaluation (DPE) Score
Sheet, visit dmv.ca.gov/teendriver. For a sample of the Supplemental/
Area DPE Score Sheet, visit dmv.ca.gov/seniors.

8
SECTION 4. Changing, Replacing, and Renewing
Your Driver’s License
Changes to Your License
If you legally change your name or need an update to your driver’s
license, such as your physical description or gender identity, visit
dmv.ca.gov/dlservices.
Change Your Address
If you move, you must notify DMV of your new address within ten days.
Submit a change of address online at dmv.ca.gov/addresschange or
by mail. It is your responsibility to ensure DMV has your correct mailing
address on record.
You do not automatically get a new driver’s license when you change
your address. You may request a replacement for a fee.
Replace or Renew Your Driver’s License
It is against the law to drive with an expired driver’s license. To
renew or replace a lost, stolen, or damaged driver’s license, visit
dmv.ca.gov/dlservices, or DMV office.
Before DMV can issue you a driver’s license, you may need to provide
additional proof of your identity. Your driver’s license and identity
document may expire on the same date. If so, you will be required to
provide a valid identity document. If you are a minor, your parent or
guardian must sign the application. Once you receive your replacement
card, your old card is no longer valid. If you nd the old card, destroy it.
Extend Your Driver’s License
If you are out-of-state and cannot renew, you may request a one
year extension of your driver’s license. Before your driver’s license
expires, submit a request with your name, driver’s license number,
birth date, California residence address, and out-of-state address to
dl-extensions@dmv.ca.gov.
NOTE Limited-term driver’s licenses are not eligible for this extension.

9
SECTION 5. An Introduction to Driving
Your health may affect your driving.
Vision – You must be able to notice hazards in different types of lighting,
judge distances, adjust to traffic speed, and read road signs.
Hearing – You must be able to hear horns, sirens, motorcycles, or
screeching tires that may alert you of hazards. It is illegal to wear a
headset or earplugs in both ears while driving.
Fatigue and Drowsiness – Can affect your vision and increase reaction
time to hazards.
Physical and Mental – You must be alert to quickly decide the correct
course of action in any type of traffic situation, including unexpected
ones.
Medications – Prescription and over-the-counter medications can make
you an unsafe driver. Some medicines can make you sleepy. It is your
responsibility to know the effects of the medications you take.
Health – Physicians are required to report patients, who are at least 14
years old, to DMV if they believe you have medical conditions that may
affect your ability to drive safely, such as lapse of consciousness.
Controlling the Vehicle
To control your vehicle, it is critical to keep both hands on the wheel
whenever possible.
Hand-to-Hand Steering (Push/Pull)
To use this steering wheel method:
1. Start with your hands at 9 and 3 o’clock or 8 and 4 o’clock.
2. Do not cross your hands over the middle of the steering wheel.
3. Keep your hands in these positions, even when making turns.

10
Hand-Over-Hand Steering
Use this steering wheel method when you turn at low speeds, park, or
need to recover from a skid. To use this method:
1. Start with your hands at 8 and 4 o’clock.
2. Reach across the steering wheel to grasp the opposite side.
3. Let go of the steering wheel with your other hand.
4. Reach across the arm still holding the wheel, grip the wheel, and pull
up.
One-Hand Steering
There are only two situations that may require steering with one hand:
• When you are turning while backing up to see where you are going
behind you. Place your hand at the 12 o’clock position on the steering
wheel.
• When you are operating vehicle controls that require you to remove a
hand from the steering wheel.
S, H, A H
Your signals, horn, and headlights are important for communicating with
other drivers, pedestrians, and bicyclists.
Signaling
Always signal when you turn, change lanes, slow down, or stop.
You can signal using your vehicle’s signal lights or using hand-and-arm
positions. If your signal lights are not functioning, or bright sunlight makes
your signal lights hard to see, use the hand-and-arm signals shown in the
image below.
Bicyclists may signal a turn with their arm held straight out, pointing in
the direction they plan to turn.
Left Turn Right Turn
Slow or Stop

11
You should signal:
• At least 100 feet before you turn.
• Before every lane change.
• At least ve seconds before you change lanes on a freeway.
• Before pulling next to the curb or away from the curb.
• Even when you do not see other vehicles around you.
• When you are almost through the intersection if you plan to turn
shortly after crossing the intersection.
Remember to turn off your signal when you no longer need it.
Using Your Horn
Use your vehicle’s horn to let other drivers know you are there or warn
others of a hazard. Use your horn to:
• Avoid collisions.
• Alert oncoming traffic on narrow mountain roads where you cannot
see at least 200 feet ahead.
Using Your Headlights
Your vehicle’s headlights help you see what is in front of you. They also
make it easier for other drivers to see your vehicle. Dim your high-beam
headlights to low beams within 500 feet of a vehicle coming toward you
or within 300 feet of a vehicle you are following. It is illegal to drive using
only parking lights. Use your headlights:
• When it is too dark to see from 1,000 feet away.
• Beginning 30 minutes after sunset.
• Until 30 minutes before sunrise.
• In adverse weather. If you need to use your windshield wipers due to
fog, rain, or snow, you must turn on your low-beam headlights.
• When conditions (such as clouds, dust, smoke, or fog) prevent you
from seeing other vehicles.
• On mountain roads and tunnels (even on sunny days).
• When a road sign states that headlights must be on.
• To help other drivers see your vehicle, especially when the sun is low
on the horizon.

12
Using Your Emergency Flashers
If you can see a collision or hazard ahead, warn drivers behind you using
these methods:
• Turn on your emergency ashers.
• Lightly tap your brake pedal three or four times.
• Use a hand signal when slowing and stopping.
If you need to stop because of vehicle trouble:
• Turn on your emergency ashers. If your vehicle does not have
emergency ashers, use your turn signals.
• If possible, pull off the road away from all traffic.
• If you cannot get completely off the road, stop where people can see
you and your vehicle from behind.
• Do not stop just over a hill or just around a curve. Other drivers may
not see your vehicle in time to avoid a collision.
• Call for emergency roadside assistance and stay in your vehicle until
help arrives.

13
SECTION 6. Navigating the Roads
T L
A traffic lane is a section of road for a single line of traffic.
Lane Markings
Lane markings on road surfaces help drivers know which part of the road
to use and understand traffic rules.
Single Solid Yellow Line
A single solid yellow line marks the center of a road with two-way traffic.
Do not pass a vehicle in front of you if there is only one lane of traffic
going your direction and a solid yellow line on your side of the road.
Double Solid Yellow Lines
Do not pass over double solid
yellow lines. Stay to the right of
these lines unless you are:
• In a high-occupancy vehicle
(HOV) carpool lane that has a
designated entrance on the
left.
• Instructed by construction or other signs to drive on the other side of
the road because your side is closed or blocked.
• Turning left across a single set of double yellow lines to enter or exit a
driveway or private road or make a U-turn.
Two sets of solid double yellow lines spaced two or more feet apart are
considered a barrier. Do not drive on or over this barrier, make a left turn,
or make a U-turn across it, except at designated openings.
Broken Yellow Line
A broken yellow line indicates you may pass if the broken line is next to
your driving lane. Only pass when it is safe.
Single Solid White Line
A single solid white line marks traffic lanes going in the same direction.
This includes one-way streets.

14
Double Solid White Lines
Double solid white lines indicate a lane barrier between a regular use
and a preferential use lane, such as a carpool (HOV) lane. You may also
see double solid white lines in or near freeway on and off ramps. Never
change lanes over double solid white lines. Wait until you see a single
broken white line.
Broken White Lines
Broken white lines separate traffic lanes on roads with two or more lanes
in the same direction.
End of Lane Markings
Ending freeway and street lanes are usually
marked with large broken lines. If you are
driving in a lane marked with broken lines, be
prepared to exit the freeway or for the lane
to end. Look for a sign that tells you to exit or
merge.
Yield Line
A yield line is a solid white line of triangles
that shows approaching vehicles where to
yield or stop. The triangles point towards
approaching vehicles.

15
Choosing a Lane
Traffic lanes are often
referred to by number. The
left (or fast) lane is called the
Number 1 Lane. The lane to
the right of the Number 1
Lane is called the Number 2 Lane. Then the Number 3 Lane e
tc, .
Here are some tips for choosing a lane:
• Use the left lane to pass or turn left.
• Use the right lane to enter or exit traffic or when you enter the road
from a curb or shoulder.
Changing Lanes
Before you change lanes:
• Signal.
• Check your mirrors.
• Check traffic behind and beside you.
• Look over your shoulder in the direction you plan to move to make
sure the lane is clear.
• Check your blind spots for other vehicles, motorcyclists, and
bicyclists. Do not let the vehicle drift into another lane.
• Be sure there is enough space for your vehicle in the next lane. It is
not necessary to slow down before a lane change.
Stay in one lane as much as possible. Do not weave in and out of traffic.
Last minute lane or direction changes may increase the risk of collisions.
Once you start moving through an intersection, keep going. If you start
to make a turn, follow through. If you miss a turn, keep driving until you
can safely and legally turn around.
Types of Lanes
Passing Lanes
On a multilane road, the passing lane (far left lane) is the lane closest to
the center divider and is used to pass other vehicles.
Carpool/High-Occupancy Vehicle (HOV) Lanes
Example of numbered traffic lanes.
An HOV lane is a special lane reserved for carpools, buses,
motorcycles, or low-emission vehicles with decals. To use an
HOV lane, one of these must apply:
16
• You have a certain number of people in your vehicle. There will be
signs at the on-ramp or along the road to tell you the minimum
number of people. Road signs also list the hours when the HOV rules
apply.
• You are driving a low emission or zero emission vehicle. You must
display a special DMV-issued decal.
• You are riding a motorcycle (unless otherwise posted).
The road surface in an HOV lane is marked with a diamond symbol and
the words Carpool Lane. Do not cross over double solid lines to enter or
exit an HOV lane. Use designated entrances and exits.
Center Left Turn Lanes
A center left turn lane is located in the middle of a two-way street. It is
marked on both sides by two painted lines. The inner line is broken and
the outer line is solid. Use the center left turn lane to prepare for and
make a left turn or U-turn. It is not a regular traffic lane or passing lane.
You may only drive for 200 feet in the center
left turn lane. To turn left from this lane:
• Look for other vehicles coming toward you
in the center left turn lane.
• Signal.
• Look over your shoulder to check your blind
spots.
• Merge completely into the center left turn
lane so you do not block traffic.
• Turn when it is safe.
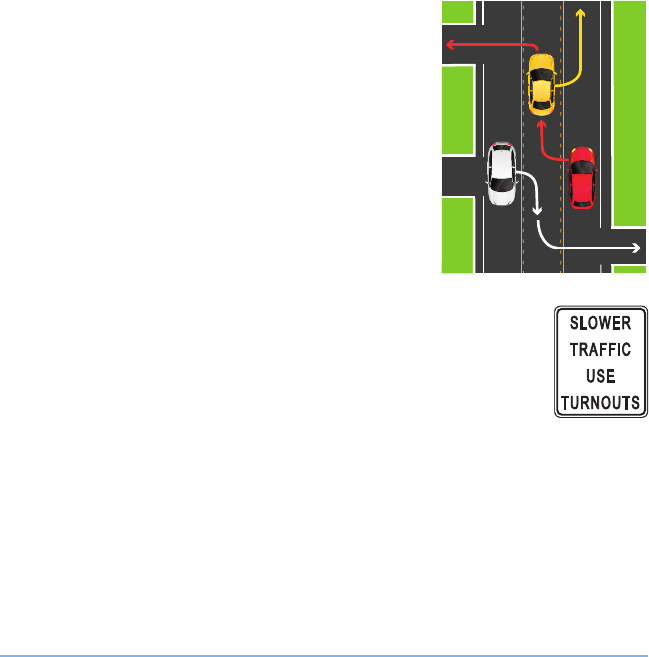
Turnout Areas or Lanes
Some two-lane roads have special turnout areas or lanes.
Merge into these areas or lanes to allow cars behind you to
pass.
You must use a turnout area or lane to let other vehicles
pass when you are driving slowly on a two-lane road, where
passing is unsafe, and there are ve or more vehicles following you.

17
Bicycle Lanes
Bicycle lanes are for bicyclists only and run alongside vehicle traffic.
They are typically marked by a single solid white line and signs. They are
sometimes painted bright green to make them easier to see.
It is illegal to drive in a bicycle lane unless you are:
• Parking (where permitted).
• Entering or leaving the road.
• Turning (within 200 feet of an intersection).
There are multiple types of bike lanes and markings:
• Bike lane: Established along streets adjacent to vehicle traffic.
Typically marked by a single solid white line that turns into a dash-line
near an intersection.
• Buffered bike lane: Uses chevrons or diagonal markings to provide
greater separation from traffic and on-street parking.
• Bike route: Uses bike route signs and shared road markings to
designate a preferred route for bicyclists on streets shared with
vehicle traffic.
• Bicycle boulevard: Prioritizes bicycle travel on streets shared with
vehicle traffic.
• Separated bikeway: Is physically separated from motor vehicle traffic
and for exclusive use of bicyclists. They are also known as a cycle
track or protected bike lanes. The separation may include exible
posts, grade separation, inexible barriers, or on-street parking.
• Shared roadway bicycle markings Alert
drivers that bicyclists can occupy the lane
and help bicyclists maintain a safe lane
position in traffic.
:
NOTE Check your blind spots before entering
a bike lane. If you drive a motorized bicycle,
use caution to avoid other bicyclists. Travel at
a reasonable speed and do not endanger the
safety of other bicyclists.
3 FEET
SHARE THE ROAD
SHARROWS
Example of shared roadway.

18
T
Right Turns
To make a right turn:
• Drive close to the right edge of the
road.
— If a designated right turn lane is
available, enter at the opening.
— You can drive in a bike lane
within 200 feet from the turn. Check for bicyclists in your blind
spots.
• Watch for pedestrians, bicyclists, or motorcyclists between your
vehicle and the curb.
• Start signaling about 100 feet before the turn.
• Look over your right shoulder and reduce your speed.
• Stop behind the limit line. A limit line is a wide white line that shows
the drivers where to stop before an intersection or crosswalk. If there
is no limit line, stop before you enter the crosswalk. If there is no
crosswalk, stop before you enter the intersection.
• Look both ways (left-right-left) and turn when it is safe.
• Complete your turn in the right lane. Do not turn wide into another
lane.
Right Turn Against a Red Light
You may turn right at a red light after a complete stop unless there is a
No Turn on Red sign. Follow the same steps listed above for right turns.
Right Turn Against a Red Arrow
You may not turn right if you are stopped at a red arrow light. Wait until
the light changes to green before making your turn.
Right Turn at a Public Transit Bus Lane
It is illegal to drive, stop, park, or leave a vehicle in an area designated for
public transit buses. Signs will be posted to indicate the lanes are for bus
only use. However, you may cross a bus lane to make a right turn.
Example of a right turn.

19
Right Turn onto a Road with a Dedicated Lane
A dedicated right turn lane does not
merge into another lane and allows you
to make a right turn without stopping.
You may make your turn even if there
is a red light for vehicles going straight
through the intersection. If there is a
traffic light or sign on the right curb of
the right turn lane, you must obey that
light or sign. Always yield to pedestrians
in a crosswalk when turning.
Left Turns
To turn left:
• Drive close to the center divider
or into the left turn lane.
— Enter a designated left turn
lane at the opening. Do not
cross any solid line.
— Enter a two-way center left turn lane within 200 feet of the turn.
Respect the right-of-way of any vehicle, bicyclist, or motorcyclist
already in the lane. Always yield to pedestrians.
• Start signaling 100 feet before the turn.
• Look over your left shoulder and reduce your speed.
• Stop behind the limit line. If there is no limit line, stop before you
enter the crosswalk. If there is no crosswalk, stop before you enter the
intersection.
• Look both ways (left-right-left) and begin your turn when it is safe.
• Proceed into the intersection while turning to complete your turn in
the left lane.
• Do not turn the steering wheel too soon and enter the lane of
oncoming vehicles.
— Keep your wheels pointed straight ahead until it is safe to start
your turn. If your wheels are pointed to the left and a vehicle hits
you from behind, you could be pushed into oncoming traffic.
• Accelerate smoothly during and after the turn.
• Allow the steering wheel to straighten in the new lane.
Example of a left turn.

20
Left Turn Against a Red Light
You may turn left against a red light when you are turning from a one-
way street onto a one-way street. Make sure there is no sign prohibiting
the turn. Yield to other vehicles, pedestrians, or bicyclists who have a
green light. Look both ways and turn when it is safe.
U-turns
A U-turn is when you turn your vehicle around to go back in the direction
you came. To make a U-turn, signal and use the left turn lane or far-left
lane. You may make a U-turn:
• Across a double yellow line.
• In a residential district if no vehicles are approaching you within 200
feet.
• At an intersection on a green traffic light or green arrow, unless a No
U-turn sign is posted.
• On a divided highway if a center divider opening is provided.
Never make a U-turn:
• Where a No U-turn sign is posted.
• At or on a railroad crossing.
• On a divided highway by crossing a dividing section, curb, strip of
land, or two sets of double yellow lines.
• When you cannot see clearly for 200 feet in each direction.
• On a one-way street.
• In front of a re station. Never use a re station driveway to turn
around.
• In business districts (the part of a city or town where most offices and
businesses are).

21
Examples of Turns
The descriptions below refer to the numbers next to the cars in the
images. Watch for pedestrians, motorcycles, and bicycles between your
vehicle and the curb. When making turns, there may be signs or arrows
that indicate you can turn from or end in more than one lane.
1. Left turn from a two-way street.
Start the turn in the left lane
closest to the middle of the street.
To reduce the risk of collision, end
the turn in the left lane closest to
the middle of the street going in
your vehicle’s direction.
1
1
2
2. Right turn. Begin and end the
turn in the lane closest to the right
edge of the road. Do not swing
wide into another lane of traffic.
3. Left turn from a two-way street
onto a one-way street. Start the
turn from the lane closest to the
middle of the street (far-left lane).
If there are three or more lanes in
your direction of travel, you may
end your turn in any lane that is
open.
3
4
3
4. Left turn from a one-way street
onto a two-way street. Start
the turn from the far-left lane. To
reduce the risk of collision, end the
turn in the left lane closest to the
middle of the street going in your
vehicle’s direction.

22
5. Left turn from a one-way street onto a
one-way street. Start the turn from the
far-left lane. Bicyclists can legally use the
left turn lane for their left turns. If there are
three or more lanes in your direction of
travel, you may end your turn in any lane
that is open.
5
6. Right turn from a one-way street onto a
one-way street. Start the turn in the
far-right lane. If safe, you may end the turn
in any lane.
6
7. Turn at a “T” intersection from
a one-way street onto a two-way
street. Traffic going straight through
the intersection has the right-of-way.
You may turn either right or left from
the center lane.
7
Braking
• Remove your foot from the gas pedal (accelerator) and allow the
vehicle to slow down. Lightly press the brake until you come to a full
stop. Give yourself enough space and time to perform this maneuver.
• When stopping at a limit line, do not cross over the line. If stopping
behind a vehicle, leave enough space to see their rear wheels.

23
M A E
Merging
Highway traffic has the right-of-way. For more information, see Right-of-
Way Rules: Who Goes First in Section 7. When you enter a highway, you
will need to:
• Be in the proper lane on the on-ramp.
• Be at or near the speed of traffic.
• Merge into highway traffic when safe to do so. Do not stop unless
absolutely necessary.
• Merge into a space large enough for your vehicle to safely join the
lane.
• Use your mirrors and turn signals.
• Turn your head quickly to look over your shoulder before changing
lanes or merging into traffic.
• Make sure you can stop safely by leaving three seconds of space
between you and the vehicle in front of you.
• Do not cross over any solid lines when merging. If you need to cross
several lanes, signal and cross them one at a time. Check your blind
spots for vehicles, motorcyclists, bicyclists, and pedestrians each time.
Exiting
To exit a highway safely:
• Know your exit and be aware of when it is approaching.
• If you plan to change lanes, do so one at a time. Signal and look over
your shoulder to check your blind spots.
• When in the proper lane, signal ve seconds (approximately 400 feet)
before you exit.
• Make sure you are at a safe speed to exit.
• Do not cross over any solid lines when exiting.

24
Crossing or Entering Traffic
When entering traffic from a full stop, signal and leave a large enough
space to get up to the speed of traffic. To merge, enter, or exit traffic, you
need a space that is:
• Half a block on city streets, which is about 150 feet.
• A full block on the highway, which is about 300 feet.
Even if you have a green light, do not start across the intersection if there
are pedestrians or vehicles blocking your pathway.
When turning left, do not assume that an oncoming vehicle with its right
turn signal on is turning before it reaches you. The driver may have their
signal on by mistake or plan to turn just beyond you. Wait for the vehicle
to start its turn before beginning the left turn.
P
You must judge whether you have enough space to pass whenever you
approach:
• An oncoming vehicle or bicyclist.
• A hill, curve, intersection, or road obstruction. To safely pass, the hill or
curve should be at least one-third of a mile ahead.
Before you pass, look ahead for road conditions that may cause other
vehicles to move into your lane.
Do not pass:
• If you are approaching a hill or curve and cannot see if other traffic is
approaching. This is very dangerous on one and two lane roads.
• Within 100 feet of an intersection, bridge, tunnel, railroad crossing, or
other hazardous area.
• At crossroads and driveways.
• Unless you have enough space to return to your lane.

25
How to Pass
When you are going to pass on an open highway:
• Signal that you plan on passing.
• Look over your shoulder to check your blind spots.
• Drive into the passing lane.
• Speed up to pass the vehicle.
• Signal and return to your original lane.
You may pass on the right only when:
• An open highway has two or more lanes going in your direction.
• The driver ahead of you is turning left and you can safely pass on the
right. Never pass on the left if the driver is signaling a left turn.
• You are on a one-way street.
Never drive off the paved or main-traveled part of the road to pass.
Being Passed
If a vehicle is passing you or signals that they plan on passing, allow the
vehicle to pass. Maintain your lane position and your speed.
26
P
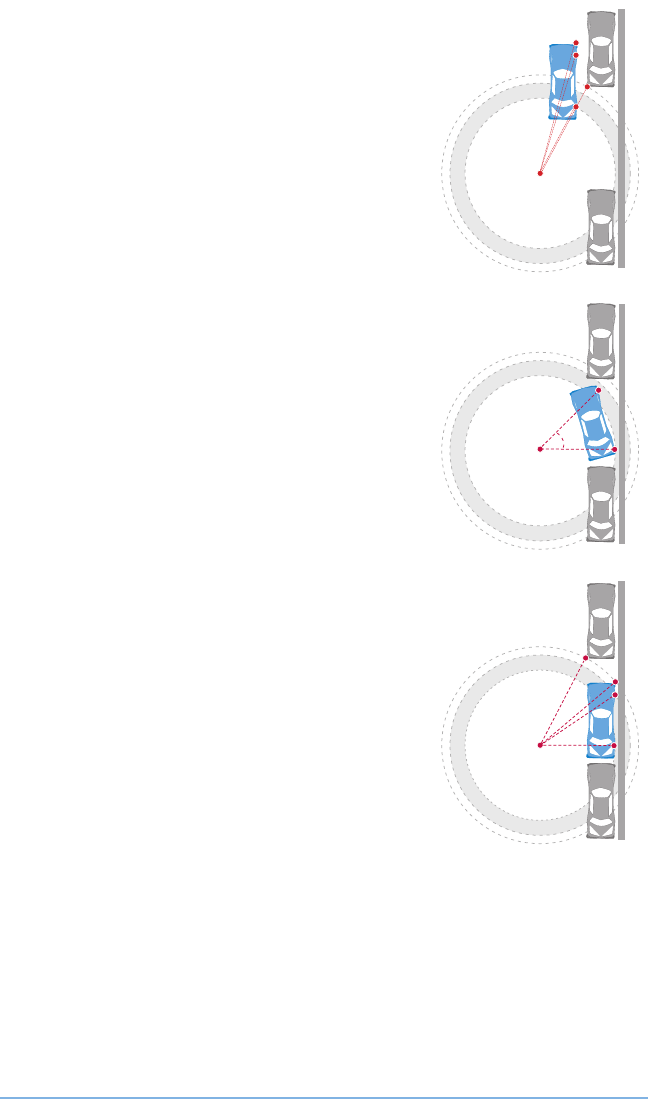
Parallel Parking
Parallel parking is when you park in line with the
road and other parked vehicles. To parallel park:
1. Find a space. Look for a space at least
three feet longer than your vehicle. When
you nd a space, turn on your signal to
show that you plan on parking.
2. Pull up alongside the vehicle in front of
the space. Leave about two feet between
your vehicle and the vehicle next to you.
Stop once your rear bumper is aligned with
the front of your parking space. Keep your
signal on.
3. Check your blind spots. Look in your
rearview mirror and over your shoulder for
approaching vehicles and pedestrians.
4. Begin backing up. Turn your steering
wheel to back into the space at about a
45-degree angle.
5. Straighten out. Begin turning the steering
wheel away from the curb when your rear
wheel is within 18 inches of the curb. You
may need to pull forward and backward to
straighten out. Your vehicle should now be
parallel and within 18 inches of the curb.
6. Parking. Turn off your vehicle and set the
parking brake. Before you exit your vehicle,
look carefully for passing vehicles, bicycles,
and motorcycles. Exit when safe.
45°

27
Straight Line Backing
To back up in a straight line:
1. Traffic check. Observe traffic and check appropriate blind spots.
2. Signal. Activate the turn signal before pulling up to the curb. Cancel
the turn signal once completed.
3. Check your blind spots. Look in your rearview mirror and over your
shoulder for approaching vehicles and pedestrians.
4. Begin backing up. Back in a straight line for three vehicle lengths
while remaining within three feet of the curb. Stay aware of what is
behind you when backing up.
5. Control. To maintain control of the vehicle, back at a smooth, safe
speed and adjust the steering wheel when needed. Practice until
you can keep the vehicle straight. Repeat steps 1 and 2 to pull away
from the curb.
Parking on a Hill
When you park on a hill, your vehicle could roll due to equipment failure.
Remember to set the parking brake and leave the vehicle in park, or in
gear for manual transmission. To park:
• On a sloping driveway:
Turn the wheels so the
vehicle will not roll into the
street, leave the vehicle in
park and set the parking
brake.
• Headed downhill: Turn your
front wheels into the curb or
right toward the side of the
road.
• Headed uphill: Turn your front wheels away from the curb (left-
towards the center of the road) and let your vehicle roll back a few
inches. The wheel should gently touch the curb.
• Headed either uphill or downhill when there is no curb: Turn the
wheels so the vehicle will roll away from the center of the road if the
brakes fail.
Downhill: turn the wheels toward the curb.
Uphill: turn the wheels away from the curb.
No Curb: turn the wheels toward the
shoulder of the road.

28
Parking at Colored Curbs
Painted colored curbs have special parking rules.
• White: Stop only long enough to
pick up or drop off passengers.
• Green: Park for a limited time. The
time limit may be posted on signs or
painted on the curb.
• Yellow: Load and unload
passengers and freight. Do not stop
longer than the time posted. If you drive a noncommercial vehicle,
you are usually required to stay with your vehicle.
• Red: No stopping, standing, or parking. Buses may stop at a red zone
marked for buses only.
• Blue: Parking for a disabled person or someone driving a
disabled person with a special placard or special license
plate.
— To learn more about disabled
parking placards and license plates,
visit dmv.ca.gov/disabled-person-
parking.
Illegal Parking
Never park or leave your vehicle:
• Where a No Parking sign is posted.
• On a marked or unmarked crosswalk.
• On a sidewalk, partially blocking a sidewalk, or in front of a driveway.
• Within three feet of a sidewalk ramp for disabled persons.
• In front of or on a curb that provides wheelchair access to a sidewalk.
• In the crosshatched (diagonal lines) area next to a designated
disabled parking space.
• In a space designated for parking or fueling zero-emission vehicles,
unless you are driving a zero-emission vehicle.
• In a tunnel or on a bridge, unless permitted by signs.
• Within 15 feet of a re hydrant or re station driveway.
• Between a safety zone and curb.
Example of crosshatched
(diagonal lines) area.

29
• Double parked.
• On the wrong side of the street or on a freeway, except:
— In an emergency.
— When a law enforcement officer requires a stop.
— Where a stop is specically permitted.
If you must stop on a freeway, park completely off the pavement and stay
in your vehicle with the doors locked until help arrives. A vehicle that is
stopped, parked, or left standing on a freeway for more than four hours
may be removed.
Electric Vehicles
Local authorities can reserve parking spaces on public
streets for electric vehicle charging.
.
D G
Maximize your fuel efficiency while helping to lower emissions
by following these practices:
• Speed up and slow down smoothly. Drive at a steady speed.
• Regularly inate your tires, get oil changes, and check lters.
• Get rid of extra weight in your vehicle.
For more information, visit fueleconomy.gov
L E S
During a Law Enforcement Stop
• Turn on your right turn signal to acknowledge that you see the officer.
• Move completely onto the right shoulder, even if in the carpool/HOV
lane. Stop in a well-lit area when possible.
• Turn off your radio.
• Remain inside your vehicle unless directed to get out by the officer.
• Roll down your window after stopping your vehicle and before the
officer makes contact with you.
• The driver and all passengers should place their hands in clear view
before the officer makes contact with them.
Beginning January 1, 2024, law enforcement officers must state the
reason for a traffic or pedestrian stop before they begin questioning
related to a criminal investigation or traffic violation. An exception is made
if an officer reasonably believes withholding the reason is necessary to
G66-21B (CA)

30
protect life or property from imminent threat. The reason for the stop
must be documented on the citation issued or law enforcement report
completed.
Your Rights During the Enforcement Stop
If an officer asks your permission to do something, you have a right to
say no. However, if you say no and the officer says they are going to do it
anyway, you do not have a right to interfere with their actions. For example,
an officer may request to search part or all of your vehicle. You have a
right to decline that request, but the officer may have the legal authority
to search your vehicle anyway under certain circumstances. If you do not
want the officer to search your vehicle, you should clearly say that you do
not give your permission, but you do not have a right to resist or obstruct
the officer if they search your vehicle anyway.
The driver of a stopped vehicle must produce a driver’s license,
proof of insurance, and vehicle registration when stopped by law
enforcement. If a driver does not produce these documents, officers
may conduct a limited search for them. An officer may also request the
names or identication of passengers. Passengers can decline that
request, but under some circumstances the passengers may be required
to identify themselves anyway. If passengers do not want to produce their
identication, they should clearly say so. Passengers should not interfere
with the officer’s duties in conducting the traffic stop, and if an officer
demands identication, passengers should not interfere with the officer’s
actions. During a traffic stop, an officer can legally require the driver and
all passengers to exit or stay inside the vehicle. If you are told to exit the
vehicle or stay inside, you must do so.
In California, only federal law enforcement officers can ask you about
your immigration status. California law prohibits state and local officers
from asking drivers or passengers about their immigration status. If a
California law enforcement officer asks you about your immigration status,
you can decline to answer.

31
In general, the First Amendment protects the right of drivers and
passengers to record interactions with law enforcement in public
spaces. If you are recording, you should immediately make that clear.
You do not have a right to interfere with the officer’s lawful duties during
the enforcement stop, and you should not reach into concealed areas
to retrieve your recording device without the officer’s permission. If your
recording is not interfering with the officer’s ability to lawfully do their job,
an officer cannot conscate your recording device, delete the recording, or
destroy the device just because you are using it to record. In general, you
also have the right to deny a request to unlock a cellular phone or provide
a password to it, though under some circumstances, such as if you are
on parole, you may have to give permission in response to such requests.
Finally, no government employee can retaliate against you just because
you recorded something in public.
Even if you believe your rights were violated, you should not engage
in physical resistance or violence against the officer. If an officer
does something that you believe violates your rights, you can voice your
objection, but you should not physically resist. Everyone has the right to
be safe during a traffic stop. Your safety and the officer’s safety could be
jeopardized if the situation escalates with physical resistance or violence.
All members of the public have a right to le a complaint against any
law enforcement agency, and it is against the law for any government
employee to retaliate against you for doing so. You can le a complaint
with the law enforcement agency that employs the officer. You
have a right to be free from discrimination based on your actual or
perceived race, sex, color, ethnicity, national origin, age, religion, gender
identity or expression, sexual orientation, mental or physical disability,
medical condition, or citizenship status. You also have other rights
guaranteed by the United States and California Constitutions, as well as
California and federal laws. When you le a complaint, the agency that
employs the officer must investigate the complaint. Links to contact
information for California law enforcement agencies can be found at
post.ca.gov/le-agencies.

DMV KIOSKS
Offer Convenient
Transactions
Available at:
Grocery Stores
DMV Offices
Complete your vehicle registration renewal
Receive a replacement registration card or sticker
Submit proof of insurance
File for planned nonoperation (PNO) status
Obtain your driver’s record and vehicle record
Receive a replacement driver’s license and more . . .
Find a kiosk near you
dmv.ca.gov/kiosks

33
SECTION 7. Laws and Rules of the Road
T C
When at or approaching traffic signals or signs, yield to pedestrians,
bicyclists, and other nearby vehicles that may have the right-of-way. See
Right of Way Rules: Who Goes First, in this section.
Traffic Signals
Solid Red Light
A red traffic signal light means STOP. You can turn right at a red
light, if:
• There is not a NO TURN ON RED sign posted.
• You stop at the stop or limit line, yield for pedestrians, and turn
when it is safe.
Red Arrow
A red arrow means STOP. Do not turn at a red arrow. Remain
stopped until a green traffic signal light or green arrow appears.
Flashing Red Light
A ashing red signal light means STOP. After stopping, you may
go when it is safe.
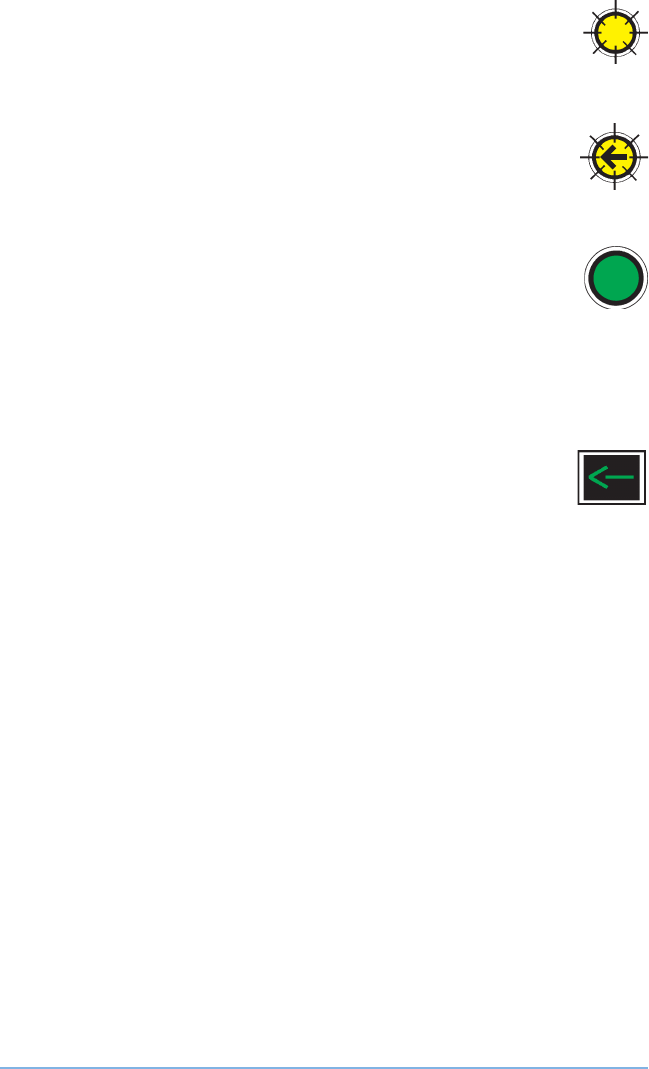
Solid Yellow Light
A yellow traffic signal light means CAUTION. The light is about
to turn red. When you see a yellow traffic signal light, stop, if you
can do so safely. If you cannot stop safely, cautiously cross the
intersection.
Yellow Arrow
A yellow arrow means the protected turning time is ending. The
signal will change soon. If you cannot stop safely or you are
already in the intersection, cautiously complete your turn. Pay
attention to the next signal. It could be a:
• Green or red traffic signal light.
• Red arrow.
34
Flashing Yellow Light
A ashing yellow traffic signal light is a warning to PROCEED
WITH CAUTION. Slow down and be alert. You do not need to
stop.
Flashing Yellow Arrow
You can turn, but your turn is not protected from other traffic.
Proceed to turn left after yielding to oncoming traffic and
proceed with caution.
Solid Green Light
A green traffic signal light means GO. You should still stop for
any vehicle, bicyclist, or pedestrian in the intersection. Only
proceed if you have enough space without creating a danger to
any oncoming vehicle, bicyclist, or pedestrian. Do not enter the
intersection if you cannot get completely across before the traffic
signal light turns red.
Green Arrow
A green arrow means GO in the direction the arrow is pointing.
The green arrow allows you to make a protected turn.
Oncoming vehicles are stopped by a red traffic signal light.
Traffic Light Not Working
When a traffic light is not working, stop as if the intersection
is controlled by STOP signs in all directions. Then proceed
cautiously when it is safe to do so.

35
Pedestrian Signals or Signs
WALK or Walking Person
You may cross the street.
DON’T WALK or Raised Hand
You may not cross the street.
Flashing DON’T WALK or Flashing Raised Hand
Do not start crossing the street. The traffic signal light is about
to change. Drivers must yield to pedestrians, even if the DON’T
WALK light is ashing.
Numbers
The numbers count down the seconds left for crossing the
street.
Diagonal Crossing
These are crisscross and diagonal crosswalks that allow
pedestrians to cross the intersection in any direction at the
same time. Cross only when the WALK signal allows it.
Sounds
Sounds such as beeping, chirping, or verbal messages help blind
or visually impaired pedestrians cross the street.
Pedestrian Push Button
This is used to activate the WALK or Walking Person signal.
No Pedestrian Signals
If there are no pedestrian signals, obey the vehicle traffic signals.
Signs
Obey all warning signs regardless of their shape or color.
STOP Sign
Make a full stop before entering the crosswalk or at the limit
line. If there is no limit line or crosswalk, stop before entering the
intersection. Check traffic in all directions before proceeding.
Red YIELD Sign
Slow down and be ready to stop to let any vehicle, bicyclist, or
pedestrian pass before you proceed.

36
Hazardous Load Placards
Red and White Regulatory Signs
No U-Turn No Left Turn No Right Turn
White Regulatory Signs
NO
PARKING
ANY
TIME
ONE
WAY
DO NOTDO NOT
BLOCKBLOCK
INTERSECTIONINTERSECTION
3
Highway Construction and Maintenance Signs
Guide Signs
Hazardous Loads Placards Slow Moving Vehicle

37
Warning Signs
Slippery
When Wet
Merging
Traffic
Divided
Highway
Two Way
Traffic
Lane Ends End Divided
Highway
Traffic Signal
Ahead
Pedestrian
Crossing
Added Lane Crossroad Stop Ahead Yield Ahead
Directional
Arrow
Curve
T
Intersection
Winding Road
For more information, visit
dot.ca.gov.

38
Red and White Regulatory Sign
DO NOT
ENTER
Follow the sign’s instruction. For example, DO NOT ENTER
means do not enter the road or ramp where the sign is posted.
WRONG WAY Sign
WRONG
WAY
If you enter a roadway against traffic, DO NOT ENTER and
WRONG WAY signs may be posted. When it is safe, back out
or turn around. If you are driving at night, you will know you
are going the wrong way if the road reectors shine red in your
headlights.
Red Circle with a Red Line Through It
The picture inside the circle shows what you cannot do and
may be shown with words.
Yellow and Black Circular Sign or X-shaped Sign
RR
You are approaching a railroad crossing. Look, listen, slow
down, and prepare to stop. Let any trains pass before you
proceed.
Many railroad crossings also have a blue and white sign to tell
you what to do if there is an emergency on or near the tracks,
or if your vehicle has stalled on the tracks.
5-sided Sign
You are near a school. Drive slowly and stop for children in the
crosswalk.
Diamond-shaped Sign
Warns you of specic road conditions and dangers ahead.
White Rectangular Sign
Communicates many important rules you must obey.
Warning Signs
Warns of conditions related to pedestrians, bicyclists, schools,
playgrounds, school buses, and school passenger loading zones.
For more information about signs, visit dot.ca.gov/programs/safety-
programs/sign-charts.

39
R--W R: W G F?
Right-of-way rules help you understand who goes rst when vehicles,
pedestrians, and bicyclists meet on the road. The vehicle that arrives to
the intersection rst has the right-of-way. Other vehicles, bicyclists, and
pedestrians must wait for the person who has the right-of-way. Never
assume that other drivers will give you the right-of-way. Give up your
right-of-way when it will help prevent collisions.
Intersections
An intersection is any place where one road meets another road.
Controlled intersections have signs or traffic signal lights. Uncontrolled
and blind intersections do not. Before entering an intersection, look left,
right, and ahead to check for vehicles, bicyclists, and pedestrians. Be
prepared to slow down and stop if necessary. Pedestrians always have
the right-of-way. Here are some right-of-way rules at intersections:
• Without STOP or YIELD signs: The vehicle that arrives to the
intersection rst has the right-of-way. However, if a vehicle, pedestrian,
or bicyclist gets to the intersection at the same time as you, give the
right-of-way to the vehicle, pedestrian, or bicyclist on your right. If you
approach a stop sign and there is a stop sign on all four corners, stop
rst and proceed as above.
• T intersections without STOP or YIELD signs: Vehicles, bicyclists,
and pedestrians on the through road (continuing to go straight) have
the right-of-way.
• Turning left: Check for pedestrians. Give the right-of-way to any
pedestrian or approaching vehicle that is close enough to be
dangerous.
• Turning right: Always check for pedestrians crossing the street, and
motorcycles and bicycles riding next to you.
• Green traffic signal light: Proceed with caution. Pedestrians have
the right-of-way.
• Entering traffic: When entering traffic, you must proceed with
caution and yield to the traffic already occupying the lanes. It is
against the law to stop or block an intersection where there is not
enough space to completely cross before the traffic signal light turns
red.

40
Roundabouts
In a roundabout, traffic travels in one direction around a central island.
How to use a roundabout:
1. Slow down as you approach.
2. Yield to all traffic already in the roundabout.
3. Enter heading to the right when there is a big enough gap in traffic to
merge safely.
4. Watch for signs and lane markings that guide you.
5. Travel in a counter-clockwise direction. Do not stop or pass.
6. Signal when you change lanes or exit.
7. If you miss your exit, continue around until you return to your exit.
If the roundabout has multiple lanes, choose your entry or exit lane
based on your destination. This is shown in the image below. To:
1. Turn right (yellow car): Choose the right lane and exit in the right lane.
2. Go straight (red car): Choose either lane. Exit in the lane you entered.
3. Turn left: Enter and continue driving until you reach the exit in the
direction you choose (blue car).
Roundabout Examples
Right Turn
Left TurnStraight

41
Pedestrians
These are considered pedestrians or vulnerable road users:
• A person walking.
• A person traveling on something other than a vehicle or bicycle. This
includes roller skates, a skateboard, etc.
• A person with a disability using a tricycle, quadricycle or wheelchair
for transportation.
,
Tricycle Quadricycle Standard
Wheelchair
Electric
Wheelchair
Although pedestrians have the right-of-way, they also must follow the
rules of the road.
When there is a pedestrian crossing a roadway with or without a
crosswalk, you must use caution, reduce your speed, or stop to allow the
pedestrian to safely nish crossing.
Other things to keep in mind:
• Do not pass a vehicle stopped at a crosswalk. You may not be able to
see a pedestrian crossing the street.
• If a pedestrian makes eye contact with you, they are ready to cross
the street. Yield to the pedestrian.
• Always allow pedestrians enough time to safely cross a street as some
groups such as seniors, people with small children, and people with
disabilities may require extra time.
Crosswalks
A crosswalk is the part of the road set aside for pedestrians to safely
cross the road. They are often marked with white lines. School crossings
may have yellow crosswalk lines. Not all crosswalks are marked.
Pedestrians have the right-of-way in marked or unmarked crosswalks. If
there is a limit line before the crosswalk, stop at the limit line and allow
pedestrians to cross the street.
Some crosswalks have ashing lights. Whether or not the lights are
ashing, look for pedestrians and be prepared to stop.

42
Pedestrians Who Are Blind
Pedestrians using guide dogs or white canes have the right-of-way at all
times. These pedestrians are partially or totally blind. Be careful when you
are turning or backing up. This is particularly important if you are driving
a hybrid or electric vehicle because blind pedestrians rely on sound to
know there is a vehicle nearby.
• Do not stop in the middle of a crosswalk. This could force a blind
pedestrian to walk into traffic outside of the crosswalk.
• Do not honk your horn at a blind person.
• When a blind person pulls in their cane and steps away from the
intersection, this gesture usually means you may go.
Mountain Roads
If two vehicles meet on a steep narrow road and neither vehicle can
pass, the vehicle facing uphill has the right-of-way. The vehicle facing
downhill has more control when backing up the hill. The vehicle facing
downhill should back up until the vehicle going uphill can pass.
S R
Drivers need to share the road with other vehicles, pedestrians, bicyclists,
road workers, and large vehicles.
Blind Spots (the No Zone)
The shaded areas in this
image are the truck driver’s
blind spots.
Large vehicle and truck drivers have a better
view in front of them and bigger mirrors.
But they also have large blind spots, also
called No Zones. In these areas, your vehicle
can disappear from a large vehicle or truck
driver’s view. If you cannot see the truck’s side
mirrors, the truck driver cannot see you.
Braking
Large vehicles and commercial trucks take
longer to stop than passenger vehicles
traveling at the same speed. When traveling,
they create extra space in front of their
vehicle to use if they need to stop suddenly. The average passenger
vehicle traveling at 55 mph can stop within 300 feet. A large vehicle
traveling at the same speed can take up to 400 feet to stop. The heavier
the vehicle and the faster it is moving, the longer it takes to safely stop,
so a loaded truck will take longer to stop than an empty truck. Do not

43
move in front of a large vehicle and suddenly slow down or stop. The
large vehicle will not be able to stop fast enough to avoid crashing into
you.
Turning
When a vehicle turns, the rear wheels follow a shorter path than the front
wheels. The longer the vehicle, the greater the difference in the length of
the turning path. This is why large vehicles and truck drivers must often
swing wide to complete a turn. When you follow a large vehicle, look at
its turn signals before you start to pass. It may appear to be turning one
direction but instead is swinging wide in the opposite direction in order
to turn.
Maneuvering
Large vehicles and trucks are not as easy to maneuver as passenger
vehicles. On a divided highway with four or more traffic lanes in one
direction, they may be driven in the two lanes farthest to the right. When
driving near large vehicles and trucks, do not:
• Change lanes directly in front of them to reach an exit or turn.
• Drive next to them longer than you need to. Always pass a large
vehicle on the left side. After you pass the large vehicle or truck,
move ahead of it. Driving alongside a large vehicle makes it hard for
the driver to avoid dangers in the road.
• Follow too closely. Tailgating decreases a vehicle’s safety distance.
• Underestimate their size and speed as they often appear to be
traveling slower.
Buses, Streetcars, Trolleys
Safety zones are spaces set aside
for pedestrians waiting for buses,
streetcars, and trolleys. Safety zones are
marked by raised buttons or markers
on a road. Do not drive through a safety
zone under any condition.
When a bus, streetcar, or trolley is
stopped at a safety zone or traffic light
you may pass at no more than 10 mph.
Safety zones are marked by dotted
white lines.
,

44
Do not overtake and pass a light rail vehicle or streetcar on the left side,
whether it is moving or standing, unless:
• When the tracks are so close to the right side that the passenger
vehicle cannot pass on the right.
• You are on a one-way street.
• A traffic officer directs you to pass on the left.
Light Rail Vehicles
On public roads light rail vehicles have
the same rights and responsibilities as
other vehicles. To safely share the road
with light rail vehicles:
• Be aware of where they operate.
Buildings, trees, and other items can
cause blind spots for the operator.
• Never turn in front of an
approaching light rail vehicle.
• Maintain a safe distance.
• Check for approaching light rail vehicles before you turn across the
tracks. Complete your turn only when the traffic light indicates you
may proceed. Be aware they can interrupt traffic lights.
,
Motorcycles
Motorcyclists have the same rights and responsibilities as other vehicle
drivers. To safely share the road with motorcyclists:
• Check for motorcycles and use your mirrors when you change lanes
or enter a road. Motorcycles are smaller in size and harder to see so
they easily disappear in vehicle blind spots.
• Allow a safe three-second following distance. This space will help you
avoid hitting a motorcyclist if they brake suddenly or fall.
• Whenever possible, give a motorcycle the full lane. It is legal to share
lanes with motorcycles, this is known as lane splitting.
• Never try to pass a motorcycle in the same lane as you.
• Check for motorcyclists before you open your door next to traffic.
• When possible, move to one side of your lane to give motorcyclists
more room to pass.
Road conditions can cause motorcyclists to suddenly change speed or
direction.
Do not turn in front of light rail
vehicles.

45
Emergency Vehicles
Give the right-of-way to any
law enforcement vehicle, re
engine, ambulance, or other
emergency vehicle using a
siren and red lights. Failure to
pull over may result in a ticket.
Drive to the right edge of the
road and stop until the emergency vehicle(s) have passed.
When approaching a stationary emergency vehicle with ashing
emergency signal lights (hazard lights), move over and slow down.
If you are in an intersection when you see an emergency vehicle,
continue through the intersection. Drive to the right as soon as it is safe
and stop.
Obey any direction, order, or signal given by a law enforcement officer,
or reghter. Follow their orders even if they conict with existing signs,
signals, or laws.
It is against the law to follow within 300 feet of any re engine, law
enforcement vehicle, ambulance, or other emergency vehicle when their
siren or ashing lights are on.
You can be arrested if you drive to the scene of a re, collision, or other
disaster. When you do this, you are getting in the way of reghters
ambulance crews, or other rescue and emergency personnel.
,
Slow-moving Vehicles
They can take longer to get up to speed
when entering traffic. Large trucks,
bicycles, and some cars lose speed on
long or steep hills. Some slow-moving
vehicles have an orange and red triangle
on their back, such as road maintenance
vehicles which usually travel at 25 mph or
less.
Yield to emergency vehicles.
An example of a slow-moving
vehicle.
,

46
Other types of slow-moving motorized vehicles that may operate on
public roads include:
• Scooters
• Neighborhood electric vehicles
• Golf carts
Adjust your speed to share the road with these vehicles.
Neighborhood Electric Vehicles (NEVs) and Low-speed
Vehicles (LSVs)
Watch for slow-moving vehicles when you see these signs or markings:
• NEV USE ONLY
• NEV ROUTE
NEVs and LSVs reach a maximum speed of 25 mph. They are restricted
from roads where the speed limit is greater than 35 mph.
Animal-drawn Vehicles
Horse-drawn vehicles and people riding horses or other animals are
allowed to share the road with motor vehicles. It is against the law to
intentionally scare horses or livestock.
Near Animals
If you see a sign with a picture of an animal, watch for animals on or near
the road. If you see animals or livestock near the road, slow down or stop
and proceed when it is safe. Be sure to follow directions from the person
in charge of the animals.
Bicycles
Bicyclists have the same rights and responsibilities as other drivers.
Bicyclists may:
• Legally ride on certain sections of freeways where there is no
alternate route and bicycling is not forbidden by law.
• Move left to avoid hazards. These may include parked or moving
vehicles, bicycles, animals, or trash.
• Choose to ride near the left curb or edge of a one-way street.
• Choose to use crosswalks by stopping and crossing as a pedestrian.

47
Bicyclist Responsibilities
As a bicyclist, you must:
• Obey all traffic signs, signal lights,
and basic right-of-way rules.
• Ride in the same direction as traffic.
• Always look over your shoulder to
make sure the lane is clear before
turning or changing lanes.
• Yield to pedestrians.
• Wear a helmet (if under 18 years
old).
• Stay visible (for example, never
weave between parked vehicles).
• Ride as near to the right curb or
edge of the roadway as possible.
• Not ride on the sidewalk (unless
allowed by the city).
• Make left and right turns in the
same way drivers do, using hand
signals and turn lanes.
• Use a bike lane, whenever possible, or use a through traffic lane.
• Have fully functional brakes.
Bicycling at Night
When it is dark out, bicyclists should avoid wearing dark clothing. Your
bicycle must have the following equipment:
• A front lamp with a white light visible from 300 feet.
• A built-in rear red reector, solid red light, or ashing red light. This
must be visible from 500 feet.
• A white or yellow reector on each pedal, the bicyclist’s shoes, or their
ankles. These must be visible from 200 feet.
• A white or yellow reector on the front wheel, a white or red reector
on the rear wheel, or reectorized tires.
Bicycling in Travel Lanes
Bicyclists traveling slower than the ow of traffic must ride as close as
possible to the right curb or edge of the road, unless:
• Passing a vehicle or another bicycle in the same direction.
• Preparing to make a left turn.
• Avoiding a hazard or road condition.
Examples of turns for bicyclists.
Intersections with special lanes
for bicyclists.

48
• A lane is too narrow for a bicycle and a vehicle to safely travel side
by-side in the lane.
• Approaching a right turn.
• On a one-way road with two or more lanes. In this case, a bicyclist
may ride near the left curb or edge of the road.
Drivers should follow at a safe distance. When it is safe, the bicyclist
should move to a position that allows vehicles to pass.
Passing a Bicyclist
,
To safely pass a bicyclist that is in the travel lane you may need to
change to another lane. In this case, pass safely then return to your
original lane. Leave space between your vehicle and the bicyclist.
Right Wrong
,
When you cannot change lanes to pass a bicyclist, allow at least three
feet between your vehicle and the bicyclist. If you cannot give three feet
of space, do not pass the cyclist until three feet of clearance can be
given. This will help you avoid putting the bicyclist in danger. Remember
to:
• Give bicyclists enough space so they are not forced into parked
vehicles or open vehicle doors.
• Only merge toward the curb or into the bike lane when it is safe.
• Merge safely behind a bicyclist when preparing to make a turn.
• Enter a bike lane no more than 200 feet before starting a turn.
• Check for bicyclists when changing lanes or entering traffic. They
may be hidden in a vehicle’s blind spots.
• Be careful when approaching or passing a bicyclist on a two-lane
road.
-

49
Road Workers and Work Zones
You will see warning signs and message boards when there are workers,
slow-moving equipment, and closed lanes ahead.
Go through the work zone carefully by:
• Slowing down.
• Allowing extra space between vehicles.
• Expecting sudden slowing or stopping.
• Watching for drivers changing lanes.
• Avoiding distractions.
Cones, drums, or other barriers will guide you through the work zone.
Prepare to slow down or stop for highway equipment. Merge as soon as
it is safe without crossing the cones or drums. Watch for bicycles if lanes
are narrow or the shoulder is closed. Obey special signs or instructions
from workers such as aggers.
Fines and Double Fine Zones
Fines for traffic violations in a work zone can be $1,000 or more. Anyone
convicted of assaulting a highway worker faces nes of up to $2,000 and
imprisonment for up to one year.
Certain roads are chosen as Safety Enhanced-Double Fine Zones. This
is due to increased collision-related injuries and fatalities. Fines are
doubled in these zones.
Fines are also doubled in highway construction or maintenance zones
when workers are present.
Move Over and Slow Down
Drivers must move over and slow down for emergency and road work
vehicles. These include:
• Stationary emergency vehicles or tow trucks displaying ashing
amber warning lights.
• Stopped road work vehicles displaying emergency ashing or amber
warning lights.

50
Vehicles with Hazardous Loads
A diamond-shaped sign on a truck
means that the truck’s load may be
dangerous (gas, explosives etc.).
Vehicles with these signs must stop
before crossing railroad tracks.
,
Heavy Traffic or Bad Weather
You must drive slower when there is heavy traffic or bad weather. At the
same time, you should not block normal and reasonable traffic ow by
driving too slowly. If you drive faster or slower than the speed limit, you
may be cited. When another driver is close behind you and wishes to
drive faster, move to the right. If you choose to drive slower than other
traffic, drive in the right lane. Refer to Choosing a Lane in Section 6 for
more information.
Towing
You must drive in the far-right lane or a lane marked for slower vehicles
when you:
• Tow a vehicle or trailer.
• Drive a truck with three or more axles.
If no lanes are marked and there are four or more lanes in your direction,
you may only drive in the two lanes closest to the right edge of the road.
Around Children
The speed limit is 25 mph within 500
feet of a school while children are
outside or crossing the street. Some
school zones may have speed limits
as low as 15 mph. When near schools,
look for
• Bicyclists and pedestrians.
• School safety patrols or crossing
guards. Be sure to obey their directions at all times.
• Stopped school buses and children crossing the street.
— Some school buses ash yellow lights when preparing to stop to
let children off the bus. The yellow ashing lights warn you to slow
down and prepare to stop.
Hazardous Load Placards
Examples of hazardous load
placards.
All vehicles must stop for school
buses.
:

51
— When the bus ashes red lights (located at the top, front, and
back of the bus), you must stop from either direction until the
children are safely across the street and the lights stop ashing.
Remain stopped while the red lights are ashing. If you fail to stop,
you may be ned up to $1,000 and your driving privilege could be
suspended for one year.
— If the school bus is on the other side of a divided or multilane
highway (two or more lanes in each direction), you do not need to
stop.
Blind Intersections
An intersection is considered blind if it has no stop signs at any corner.
If your view is blocked, move slowly forward until you can see. The speed
limit for a blind intersection is 15 mph.
Alleys
An alley is any road no wider than 25 feet that is used to access the rear
or side entrances of buildings or properties. You may drive on or cross a
sidewalk to enter or exit a driveway or alley. The speed limit in an alley is
15 mph.
Near Railroad or Light Rail Tracks
The speed limit is 15 mph within 100 feet of a railroad crossing and you
cannot see the tracks for 400 feet in both directions. You may drive
faster than 15 mph if the crossing is controlled by gates, a warning signal,
or a agman. At railroad or train crossings:
• Flashing red warning lights indicate you must stop and wait. Do not
proceed over the railroad tracks until the red lights stop ashing, even
if the gate rises.
• When the crossing devices or a person warns you a train is coming,
stop at least 15 feet from the nearest track.
• Do not go under lowering gates or around lowered gates. If the gates
are lowered and you do not see a train approaching, call the posted
railroad emergency toll-free number or 911.
• Stop, look, and listen. If you see a train coming or hear a horn or
bell, do not cross. Many crossings have multiple tracks. Look in both
directions and only cross when it is safe.

52
• Expect a train on any track, at any time, traveling in either direction.
• Never stop on the railroad tracks. Wait and do not begin proceeding
if you do not have enough room to completely cross the tracks. If you
are on the tracks, you risk injury or death.
• Watch for vehicles that must stop before they cross train tracks.
These vehicles include buses, school buses, and vehicles marked
with a hazardous materials placard.
Business or Residential Districts
The speed limit is 25 mph, unless otherwise posted.
O I R I
You must:
• Not smoke when a minor is in the vehicle. You can be ned.
• Not dump or abandon animals on a highway. This crime is punishable
by a ne of up to $1,000, six months in jail, or both.
• Not drive a vehicle so overloaded that you cannot control it, see
ahead, or see to the sides of your vehicle.
• Not drive a vehicle with an unsecured load that is a safety hazard.
• Not carry anything in or on a passenger vehicle which extends
beyond the fenders on the left side or more than 6-inches beyond
the fenders on the right side.
— Cargo that extends more than 4 feet from the back-rear bumper
of the vehicle must display a 12-inch red or uorescent orange
square ag.
— At night, this cargo must be marked with two red lights.
• Not allow a person to ride in the back of a pickup or other truck
unless the vehicle has secure seats and seat (safety) belts.
• Not transport animals in the back of a pickup or other truck unless
the animal is properly secured. This prevents the animal from falling,
jumping, or being thrown from the vehicle.
• Not drive a vehicle equipped with a video monitor visible to the driver,
unless it only displays vehicle information, a navigation system, media
player, or radio.
• Not throw a cigarette, cigar, or other aming or glowing substance
from your vehicle.

53
• Not put signs or other objects on the front windshield or side rear
windows that block your view. Do not hang objects on the mirror.
Objects may only be affixed in these locations:
— A 7-inch square on the lower corner of the passenger’s side
windshield or the lower corner of the rear window.
— A 5-inch square on the lower corner of the driver’s side window.
— A 5-inch square located in the center uppermost portion of your
windshield for an electronic toll payment device.
— On the side windows behind the driver.
• Not interfere with a funeral procession. A funeral procession is led
by a traffic officer and has the right-of-way. All vehicles taking part in
the procession have windshield markers to identify them and have
their headlights on. You can be ticketed if you interrupt a funeral
procession.
• Not operate a vehicle with an illegible license plate.
• Not alter a license plate in any way.
Evading Law Enforcement
It is a misdemeanor to use a motor vehicle to ee or attempt to
evade law enforcement performing their duties. This is punishable by
imprisonment in a county jail for one year or less.
A person convicted of causing serious bodily injury during a law
enforcement pursuit is subject to imprisonment in a state prison for up
to seven years, or a county jail for one year or less.
A person convicted of manslaughter resulting from evading law
enforcement during a pursuit is subject to imprisonment in a state prison
for a minimum of 4 to 10 years.
If an unlicensed person is caught driving your vehicle, it may be
impounded for 30 days.
Speed Contests and Reckless Driving
A person convicted of reckless driving or engaging in a speed contest
that causes injury to another person is subject to imprisonment, a ne, or
both.
Points on Your Driver’s Record
DMV monitors your driver’s record. If you are stopped by a law
enforcement officer and cited (ticketed) for a traffic violation, you sign
the ticket as a promise to appear in traffic court. As an adult or minor,

54
if you get a traffic ticket and fail to appear (FTA) in court, DMV may
suspend your driving privilege until you appear. If you do not keep your
promise to appear in court, the FTA goes on your driver record.
Each time you are convicted of a moving traffic violation, the court
noties DMV. The conviction is placed on your driver’s record.
Convictions reported by other states and juvenile court are also added
to your driver’s record. Traffic convictions and collisions stay on your
record for 36 months or longer, depending on the type of conviction. As
an adult, your license may be suspended if your driver’s record shows
one of the following point totals:
• 4 points in 12 months.
• 6 points in 24 months.
• 8 points in 36 months.
Traffic Violator School
If you are given a one-point traffic violation, the judge may offer you the
choice to attend a traffic violator school to have the citation not reported
to your insurance company but remain on your driving record. You can
do this once in any 18-month period. The school will report your course
completion to the court. You will also get a completion receipt.
If you are a commercial driver cited in a noncommercial vehicle, see the
California Commercial Driver Handbook.
Suspension or Revocation
If you have too many points on your driver’s record, you will be
considered a negligent driver. DMV will place you on probation, suspend,
or revoke your driving privilege. When this happens, you have the right to
a hearing. DMV will notify you in writing of any action taken against your
driving privilege and inform you of your legal rights, including your right
to a hearing.
DMV will revoke your driving privilege if you are convicted of a hit-
and-run or reckless driving that resulted in injury. Courts also have the
authority to suspend a person’s driving privilege.
At the end of your suspension or revocation, you may apply for
a replacement driver’s license. You must show proof of nancial
responsibility (such as SR 22/SR 1P).

55
Maintaining Your Minor’s (Provisional) Driver’s License
If you get into collisions or commit traffic violations within the rst 12
months of obtaining your minor’s driver’s license, DMV may restrict or
suspend your driving privilege. You cannot drive if your driving privilege
is suspended or revoked.
As a minor, DMV may take action against your license if you have:
• One at fault collision or traffic violation conviction: An at fault collision
means you were found responsible.
• Two at fault collisions, two traffic violation convictions, or one of each:
You cannot drive for 30 days unless a licensed adult, at least 25 years
old, rides with you.
• Three at fault collisions, three traffic violation convictions, or a
combination: Your driving privilege will be suspended for six months.
You will be on probation for one year.
— If you have more at fault collisions or traffic violation convictions
while on probation, your license will be suspended again.
• A conviction of using alcohol or a controlled substance, or both and
are 15-20 years old: The court will order DMV to suspend your driving
privilege for one year or delay your eligibility to apply for a driver’s
license.
NOTE: Turning 18 years old does not erase or end existing restrictions,
suspensions, or probation sentences.
Administrative Hearing
Administrative hearings are conducted by DMV. If you received
notication that a proposed action is being taken against your driving
privilege, you must request a hearing within 10 days of being served or
14 days from the date the notice is mailed. If you do not make a timely
request, your right to a hearing will be lost.
This hearing provides you with an opportunity to be heard before an
action is taken against your driving privilege. You may also have to
appear in court for the same reason. Any action taken by the court is
independent of the action taken by DMV.

56
Your Hearing Rights
You have the right to:
• Present relevant evidence and witnesses on your behalf.
• Testify on your behalf or be represented by an attorney or other
representative at your expense. Representation by an attorney is not
required.
• Review the evidence and cross examine the testimony of any
witness. DMV bases its case only on written documents. If you wish
to question someone who prepared a document or is listed on a
document used as evidence, it is your responsibility to acquire a
subpoena.
For more information regarding Administrative Hearings, visit
dmv.ca.gov/driversafety.
Unsafe Driver
If you know someone who no longer drives safely, you may submit
a Request for Driver Reexamination to DMV to review their driving
qualications. To obtain a form, visit dmv.ca.gov/reexamination.
R C
Most information in your driver’s record is available to the public, except
physical or mental conditions, address, and social security number.
You can get a copy of your driver’s record online or at a kiosk. For more
information on record requests, visit dmv.ca.gov/record-requests.

57
SECTION 8. Safe Driving
B A Y S
To drive safely, you need to know what is around you. This helps you
make good decisions and react to hazards on the road. This image shows
the areas around your vehicle.
• Green: Ahead of you.
• Blue: Next to you.
• Yellow: Blinds spots.
• Red: Behind you.
Scan Your Surroundings
To give yourself time to react, avoid last minute
moves and hazards, always keep your eyes moving and scan the road at
least 10 seconds ahead of your vehicle.
Tailgating (Following Too Closely)
Tailgating makes it harder for you to see the road ahead because the
vehicle in front of you blocks your view. You will not have enough time to
react if the driver in front of you brakes suddenly. Use the three-second
rule to ensure a safe following distance and avoid a collision. Following
other vehicles at a safe distance gives you enough time to react if
another driver makes a mistake.
If a vehicle merges in front of you too closely, take your foot off the
accelerator. This creates space between you and the vehicle ahead.
Create more space in front of your vehicle when:
• A tailgater is behind you. Maintain your course and speed. Then,
when safe to do so, merge right to change into another lane and allow
the tailgater to pass.
• Following motorcyclists on metal surfaces (bridge gratings, railroad
tracks, etc.), and gravel.

58
Know What Is at Your Side
Be aware of what is on each side of you. To maintain enough space to
maneuver safely and react to other drivers:
• Do not stay in another driver’s blind spot.
• Avoid driving directly alongside other vehicles.
• Make space for vehicles entering freeways, even if you have the right-
of-way. Be ready for rapid changes and watch for signals from other
drivers.
• Keep space between your vehicle and parked vehicles.
• Look both ways, even at intersections where traffic has a red light or
stop sign.
Blind Spots
Every vehicle has blind spots. These
are areas around the vehicle that
a driver cannot see when looking
straight ahead or using the mirrors. For
most vehicles, the blinds spots are at
the sides slightly behind the driver.
To check your blind spots, look over
your right and left shoulders out of
your side windows. Only turn your head when you look. Do not turn your
whole body or steering wheel. Check your blind spots before you:
• Change lanes.
• Turn at an intersection.
• Merge with traffic.
• Back up.
• Leave a parking space.
• Parallel park.
• Pull out from the curb.
• Open your car door.
,
The shaded areas are your blind
spots.

59
Know What is Behind You
Knowing what is behind you can help you avoid rear-end collisions.
Check traffic behind you often by using your rearview mirror, side mirrors,
and turning your head when you:
• Change lanes.
• Check your blind spots.
• Reduce your speed.
• Turn into a side road or driveway.
• Stop to pull into a parking space.
• Pull up to and away from the curb.
• Back up.
U R C
Darkness
When driving at night, use your high-beam headlights on open country
roads or dark city streets. Make sure you can stop in the distance lit by
your headlights. Do not use high-beam headlights in areas where they
are illegal. Dim your high-beam headlights to avoid blinding the driver of
an oncoming vehicle. If another vehicle’s lights are too bright:
• Do not look directly into the oncoming headlights.
• Look toward the right edge of your lane.
• Watch the oncoming vehicle out of the corner of your eye.
• Do not react to the other driver by keeping your high-beam
headlights on. This only makes it harder for both of you to see.
When it is raining, use your low-beam headlights. Do not drive using only
your parking lights. When you drive at night, remember:
• Motorcycles, pedestrians, and bicyclists are much harder to see.
• Highway construction can take place at night. Reduce your speed in
highway construction zones.
• When you leave a brightly lit place, drive slowly until your eyes adjust
to the darkness.
• When a vehicle with one light drives toward you, drive as far to the
right as possible. It could be a bicyclist, motorcyclist, or vehicle with a
missing headlight.

60
Sun Glare
To help manage sun glare:
• Keep the inside and outside of your windshield clean.
• Wear polarized sunglasses.
• Maintain enough space between your vehicle and the vehicles
around you.
• Make sure your car visor works and is free of anything that would
restrict use.
• Be aware of pedestrians. You may have difficulty seeing them.
• Try to avoid driving during sunrise and sunset.
Skids
A skid is when one or more of the tires lose traction with the road and the
vehicle starts to slip. You may not be able to control your vehicle. There
are a few different types of skids.
Slippery Surface Skids
Ice and packed snow on the road can cause your vehicle to skid. This is
even more likely if you are driving too fast or going downhill. Drive slowly
and leave space between your vehicle and the vehicle ahead of you. To
prevent skidding on slippery surfaces:
• Slow down as you approach intersections and curves. For sharp
curves, slow down as you approach and move through.
• Avoid fast turns and quick stops.
• Shift to low gear before going down a steep hill.
• Avoid areas like ice patches, wet leaves, oil, or standing water.
If you start to skid, follow these steps:
1. Slowly remove your foot from the accelerator.
2. Do not use the brakes.
3. Turn the steering wheel in the direction of the skid.
4. Try to get a wheel on dry pavement.
Locked Wheel Skids
A locked wheel skid is usually caused by braking too hard when you are
going too fast. If this happens, your vehicle will skid no matter which way
the steering wheel is turned. To get out of a locked wheel skid if your
vehicle is equipped with:
• Four-wheel antilock braking system (ABS), apply rm pressure on the
brake pedal.
• Rear-wheel ABS (common in light trucks):

61
— Ease up on the brake pedal while maintaining just enough
pressure to allow the front wheels to roll again so you can steer.
— Stop braking and turn the steering wheel into the direction of the
skid.
• Front-wheel ABS, remove your foot from the brake pedal to unlock
the wheels. Steer in the direction you want to go and straighten the
front wheels as the vehicle begins to straighten out.
NOTE: To determine if your vehicle has ABS, refer to the vehicle owner’s
manual.
If your vehicle is not equipped with ABS and begins to skid, quickly pump
your brakes until you are at a safe speed. If you:
• Press the brake pedal and it sinks to the oor, quickly pump the
brakes by gently applying and releasing pressure on your brake pedal.
• Pump the brakes, down shift your vehicle into a lower or neutral gear
to slow down. Then try using your emergency brake to stop.
If your brakes get wet, you can dry them by lightly pressing the
accelerator and brake pedals at the same time. Only do this until the
brakes dry.
Slippery Roads
Rain, snow, or mud can make the roads slippery. Drive more slowly than
you would on a dry road. Adjust your speed for different conditions:
• Wet road: Reduce your speed by 5 to 10 mph.
• Packed snow: Reduce your speed by half.
• Ice: Reduce your speed to no more than 5 mph.
Some road surfaces are more slippery than others when wet. These
usually have warning signs posted. Here are situations where the road
may be more slippery:
• Shade from trees or buildings can hide icy spots on cold, wet days.
These areas freeze rst and dry out last.
• Bridges and overpasses tend to freeze before the rest of the road.
They can have icy spots.
• When it starts to rain, the pavement can be very slippery.
Slow down at the rst sign of rain, drizzle, or snow on the road. This is
especially true if it has been dry and hot for some time, because oil and
dust on the road’s surface have not been washed away.

62
Turn on your windshield wipers, low-beam headlights, and defroster. In
a heavy rainstorm or snowstorm, you may not be able to see more than
100 feet in front of your vehicle. If you cannot see farther than 100 feet,
it is not safe to drive faster than 30 mph. You may have to stop from time
to time to wipe mud or snow off your windshield, headlights, and taillights.
If you drive in snowy areas, carry snow chains for your tires. Snow chains
give your tires more traction. Carry the correct number and type of
chains for your vehicle.
Hydroplaning
Hydroplaning occurs when driving in wet or rainy conditions.
Hydroplaning is when a vehicle rides on water because the tires lose
all contact with the road. A slight change of direction, applying the
brakes, or a gust of wind could throw the vehicle into a skid. To avoid
hydroplaning:
• Drive slowly.
• Steer around standing water, if possible.
• Slow down if you hear sloshing sounds from the tires.
• Slow down when changing lanes or direction.
If your vehicle starts to hydroplane:
• Slow down gradually.
• Do not use the brakes. Sudden braking may cause you to lose control
of your vehicle.
Stuck in Snow or Mud
If stuck in the snow or mud, follow these steps:
1. Shift into a low gear and keep the front wheels straight.
2. Gently step on the accelerator. Avoid spinning the wheels.
3. Drive slowly forward as far as possible.
4. Shift into reverse and slowly back up as far as possible. Do not spin
the wheels.
5. Shift into a low gear again and drive forward.
6. Repeat a forward-backward motion until the vehicle rolls free.
7. In deep mud or snow, put boards, tree branches, etc., under the tires.
Only take this action when the vehicle is stopped.

63
Flooded Roads
Excessive water on a road may cause ooding. This can happen
gradually or suddenly. It is important to understand the dangers of water
on the road, including:
• Being swept off the road.
• Floating debris and unseen hazards.
• The road collapsing.
• Vehicle malfunction.
• Electrocution if there are fallen power lines.
It may not be possible to determine the depth of the ood by looking.
If the water is deep, the road may be too dangerous to cross. It is best
to nd another route. If you have no other option but to drive through a
ooded road, drive slowly. After you make it through the water, test your
brakes to make sure they work correctly.
High Winds
High winds can be a hazard while driving. This is especially true for larger
vehicles such as trucks, campers, and vehicles with trailers. When driving
in high winds:
• Reduce your speed. This gives you better control over your vehicle.
You will have more time to react if your vehicle gets hit by a strong
gust of wind.
• Maintain a rm hand position on the steering wheel. Strong wind
gusts are unpredictable. If you are not holding the wheel properly
and a gust hits, you can lose control of the vehicle.
• Be alert. Look ahead and watch for any debris on the road. Give
yourself enough time to react to road hazards.
• Do not use cruise control. Maintain maximum control of the
accelerator if a gust occurs.
• Be proactive. It may be safer to pull over and wait for the storm to
pass.

64
Fog or Heavy Smoke
It is best to avoid driving in heavy fog or smoke. Consider postponing
your trip until the fog clears. If you must drive in heavy fog or smoke:
• Drive slowly.
• Use your low-beam headlights. High-beam headlights will reect back
and cause glare.
• Never drive using only your parking or fog lights.
• Make sure you can stop within the space you can see ahead.
• Increase your following distance.
• Use your windshield wipers and defroster as necessary.
• Avoid crossing lanes or passing traffic unless absolutely necessary.
• Listen for traffic you cannot see.
If the fog becomes too thick to drive safely, consider pulling off the road.
Activate your emergency ashers and wait for conditions to improve.
Law Enforcement Traffic Breaks
During a traffic break, the officer turns on their emergency lights and
slowly weaves across lanes. Law enforcement uses traffic breaks to:
• Slow or stop traffic to remove hazards from the road.
• Slow or stop traffic during heavy fog or unusual traffic conditions.
• Prevent collisions during unusual conditions.
You should:
• Turn on your emergency ashers to warn other drivers.
• Slowly decrease your speed to the same speed as the officer. Do
not brake suddenly unless necessary to avoid a collision. Keep a safe
distance from the patrol vehicle ahead of you.
• Not drive past the patrol vehicle. Do not speed up until the officer
turns off their emergency lights and traffic conditions allow you to
return to your normal speed.

65
P Y Y P
Seat Belts
You and your passengers must wear seat
belts. You can get a ticket if you do not.
If your passenger is under 16 years old,
you can also get a ticket if they are not
wearing their seat belt.
Wearing the lap belt and shoulder
harness of a seat belt will increase your
chance of survival in most types of
collisions. This image shows what can
happen in a collision.
When you are in a collision, your vehicle
stops. But you keep moving at the same
speed you were traveling. You only stop
when you hit the dashboard or windshield.
If you are struck from the side, the impact
could push you back and forth across the
seat. Seat and shoulder belts keep you
in a better position to control the vehicle.
They may also minimize serious injuries.
It is important to wear the seat belt correctly to avoid injury or death:
• Wear the shoulder harness across your shoulder and chest. There
should be little to no slack. Do not wear the shoulder belt under your
arm or behind your back.
• Adjust the lap belt so that it is snug and lies low across your hips.
Otherwise you might slide out of the belt in a crash.
• If you are pregnant, wear the lap belt as low as possible under your
abdomen. Place the shoulder strap between your breasts and to the
side of your abdomen’s bulge.
IMPACT - If the red arrow
were another car hitting your
car on the driver’s side:
1. You would rst be thrown
against the driver’s side door,
2. Then you would “rebound”
and be thrown toward the
passenger’s side door.

66
Child Restraint System and Safety Seats
You must secure children with a federally-approved child passenger
restraint system or safety belt. The requirements depend on the child’s
height and age.
• Children who are under 2 years old, under 40 pounds, and
under 3 feet 4 inches tall: Secure in a rear-facing child passenger
restraint system.
NOTE A child in a rear-facing child passenger restraint system may not
ride in the front seat of an airbag-equipped vehicle.
• Children who are under 8 years old, or who are less than 4 feet
9 inches tall: Secure in a child passenger restraint system in a rear
seat. In some cases, children under 8 years old may ride in the front
seat of a vehicle in a federally-approved child passenger restraint
system. They may ride in the front seat if:
— There is no rear seat.
— The rear seats are side-facing jump seats.
— The rear seats are rear-facing seats.
— The child passenger restraint system cannot be installed properly
in the rear seat.
— All rear seats are already occupied by children 7 years old or
younger.
— Medical reasons prevent the child from riding in the back seat.
• Children who are 8 years old or older, or at least 4 feet 9 inches
tall: May use a properly secured safety belt that meets federal
standards.
Your local law enforcement agency or re department can check the
installation of your child passenger restraint system. As your child grows,
check that the child passenger restraint system is the right size.

67
Air Bags
Air bags are a valuable safety feature on many vehicles. They can help
keep you safer than a seat belt alone.
Ride at least 10 inches from the airbag cover, as long as you can maintain
full control of your vehicle. Measure from the center of the steering
wheel to your breastbone. Contact your vehicle dealer or manufacturer
if you cannot safely sit 10 inches away from the air bag. They may have
advice about additional ways to move back from your air bag. Passengers
should also sit at least 10 inches away from the passenger-side air bag.
NOTE Children seated next to a side air bag may be at risk of serious or
fatal injury.
Unattended Children and Pets
It is illegal to leave a child who is six years old or younger unattended in
a vehicle. A child may be left under the supervision of a person who is at
least 12 years old.
It is dangerous and illegal to leave children or animals in a hot vehicle.
The temperature inside a parked vehicle can rise rapidly when it is sitting
in the sun. This is true even if a window is left slightly open. Too much
exposure to heat can lead to dehydration, heat stroke, and death.
M Y S
In California, you may never drive faster than is safe for the current road
conditions. This is known as the Basic Speed Law.
Make sure you manage your speed and slow down when conditions call
for it. Regardless of the posted speed limit, your speed should depend
on:
• The number of vehicles on the road.
• The speed of other vehicles on the road.
• The road surface: smooth, rough, graveled, wet, dry, wide, or narrow.
• Bicyclists or pedestrians on or crossing the road.
• Weather: rain, fog, snow, wind, or dust.
• Traffic congestion: small changes in your driving habits can help
reduce congestion. Avoid weaving in and out of freeway lanes.
There are also situations with specic speed limit laws and conditions
where you should reduce your speed. Unless otherwise posted, the ideal
maximum speed limit on most California highways is 65 mph. It is 55 mph
on a two-lane undivided highway and for vehicles towing trailers.

68
Choose Between Hazards
Sometimes dangers will be on both sides of the road at the same time.
For example, parked cars to the right and oncoming cars to the left.
If one danger is greater than the other, give more space to the most
dangerous situation. Suppose you are on a two-lane road with an
oncoming vehicle to the left and a bicyclist ahead to your right. Instead
of driving between the vehicle and the bicyclist, take one danger at a
time. Slow down and let the oncoming vehicle pass. When the vehicle
has passed, move to the left to allow plenty of space (at least three feet)
to pass the bicyclist. If there is a steady ow of oncoming vehicles, use as
much of the left lane as you safely can to pass the bicyclist.
Know How to Handle Emergencies
There are many types of emergencies you may encounter when you
drive. Knowing how to handle emergencies can help keep you safe.
Tire Blowouts
If you have a tire blowout, do not panic or overreact. Suddenly braking
or abruptly removing your foot from the accelerator can result in a loss
of control over the vehicle. Instead, you should take the following steps
recommended by the National Highway Traffic Safety Administration:
• Hold the steering wheel with both hands.
• Maintain your vehicle speed if possible and safe.
• Gradually release the accelerator.
• Correct the steering as necessary to stabilize your vehicle and regain
control.
• Look and steer in the direction you want your vehicle to go.
• Once your vehicle has stabilized, continue to slow down and pull off
the road where and when it’s safe.
Driving Off the Pavement
If your wheels drift off the pavement:
1. Grip the steering wheel rmly.
2. Remove your foot from the accelerator.
3. Brake gently.
4. Check for traffic behind you.
5. Carefully steer back onto the pavement.
Do not pull or turn your steering wheel with too much force. This may
cause you to drive into oncoming traffic.

69
Overheating Conditions
In extreme heat, you should:
• Watch the temperature gauge.
• Avoid driving at high speeds for long periods.
• Turn off the air conditioner.
In extreme cold, you should:
• Watch the temperature gauge. The engine may not have the correct
level of antifreeze.
• Use the defroster or slightly open your windows to keep them from
fogging up.
NOTE: See the vehicle owner’s manual for more information.
If Your Vehicle Becomes Disabled on the Freeway
If your vehicle stops working on the freeway:
1. Safely pull over to the right shoulder.
2. Exit on the right side so you are away from traffic if you must get out
of the vehicle.
3. Dial 511 from your cell phone or locate a call box for assistance.
4. Return to your vehicle as soon as you can. Get back into the vehicle
from the right side (away from traffic).
5. Stay inside your vehicle with your seat belt on until help arrives.
6. Use your emergency ashers at your discretion. They can help other
vehicles see you at night and in different weather conditions.
There are certain circumstances where it is safer to get out of your
vehicle and stay away. These include situations where there is:
• Not enough space on the shoulder.
• A guardrail.
• An area for you to safely stay away from freeway lanes.
California Highway Patrol (CHP) Freeway Service Patrol (FSP)
During commute times, the CHP FSP provides free emergency roadside
services in certain areas. If you get stuck on the freeway because your
vehicle stops running, FSP will:
• Provide a gallon of gas if you run out.
• Jump start your vehicle if the battery is dead.
• Rell your radiator and tape hoses.
• Change a at tire.
• Report a collision to CHP.

70
If FSP cannot start your vehicle, they will have it towed (free of charge) to
a CHP-approved location. CHP will notify an auto club or towing service.
FSP will not:
• Tow your vehicle to a private repair service or residence.
• Recommend tow service companies or repair and body shops.
• Tow motorcycles.
• Help vehicles which have been involved in a collision, unless they are
directed to by CHP.
Call 511 for FSP information and assistance.
Disabled Vehicles on Railroad Tracks
If your vehicle stalls or stops while blocking
part of a train track with a train approaching
and warning lights ashing:
• Immediately exit your vehicle. Run away
from the tracks diagonally in the direction
the train is coming from. Then call 911.
If you do not see a train approaching and
warning lights are not ashing:
• Exit your vehicle. Dial the number located on the railroad crossing
posts or metal control box near the tracks. Provide the crossing
number (if posted). Tell them a vehicle is on the tracks. Then call 911.
D N D D
Avoid distractions while you drive. Some common distractions are:
• Looking at a phone, navigation system, children, and pets.
• Changing music or volume.
• Applying makeup or shaving.
C P T
Cell phones are the main source of distracted driving.Driving while using
a handheld cell phone is unsafe and illegal.
Adult drivers should only use a cell phone in hands-free mode when
necessary.
• Do not answer your cell phone if it rings. Let the call go to voicemail. If
you must return or make a call, pull safely off the road.
• Do not send or read text messages or emails while driving.

71
• Mount your cell phone on the windshield, dashboard, or center
console. It cannot block your view of the road.
• Use the single swipe or touch feature on the mounted cell phone.
M C P
It is against the law for a minor to use a cell phone or electronic wireless
device to answer calls and send or respond to text messages while
driving.
EXCEPTION: Minors may use a cell phone to make a call for emergency
assistance.
B F N T
The technology in vehicles is always advancing. We will see more self-
driving vehicles and vehicles with advanced driver assistance systems
(ADAS) on the road. Vehicles with these systems may respond to road
situations differently than a human driver would.
B A C M
All gas-powered vehicles produce carbon monoxide. Carbon monoxide
is a deadly odorless gas released from a vehicle’s exhaust pipe. Never
start your vehicle inside the garage with the door closed. Symptoms of
carbon monoxide poisoning include:
• Tiredness
• Yawning
• Dizziness
• Nausea
• Headache
• Ringing in the ears
If you are experiencing any of these symptoms, have your exhaust
system checked.

72
SECTION 9. Alcohol and Drugs
California’s driving under the inuence (DUI) laws apply to both alcohol
and drugs. It is illegal to drive while under the inuence of alcohol or any
drug that affects your ability to drive safely. As you age, your tolerance
to alcohol decreases, which increases the risk of alcohol-related driving
problems. The law does not see a difference between illegal drugs and
medications you get from a doctor or pharmacy. They can all affect your
ability to drive safely and react to what you see and hear.
No matter what age you are, it is illegal to drive after:
• Drinking excessive amounts of alcohol in any form. This includes
medications like cough syrup.
• Taking any drug that affects your ability to drive. This includes
prescriptions or over-the-counter medications.
• Using any combination of alcohol or drugs that decreases your ability
to drive safely.
Make sure you read medication labels and know the effects of any drug
you use. If a law enforcement officer thinks you are driving while under
the inuence of drugs or alcohol, they have the right to ask you to take a
blood or urine test. If you refuse to take one, DMV will suspend or revoke
your driving privilege for one year.
IMPORTANT: If you are 13 to 20 years old and convicted of operating
a bicycle while under the inuence of alcohol or drugs, your driving
privilege may be suspended or delayed for one year once you are
eligible to drive.
U P A C
P V
The law is very strict about carrying alcohol or cannabis products in
your vehicle with you. It is illegal to drink any alcohol, to smoke or eat
a cannabis product while you are driving or riding as a passenger in
a vehicle. If you are carrying any alcohol, cannabis in your vehicle, the
container must be sealed and unopened. If it is open, you must keep
the container in the trunk or place where passengers do not sit. It is
also illegal to keep an open container of alcohol in your glove box. This
law does not apply if you are a passenger in a bus, taxi, camper, or
motorhome.

73
B A C (BAC) L
When you consume alcohol, traces of it enter your bloodstream. Your
BAC measures how much alcohol is present in your bloodstream.
It is illegal for you to drive if you have a BAC of:
• 0.08% or higher if you are over 21 years old.
• 0.01% or higher if you are under 21 years old.
• 0.01% or higher at any age if you are on DUI probation.
• 0.04% or higher if you drive a vehicle that requires a commercial
driver’s license.
• 0.04% or higher if you are driving a passenger for hire.
If you drive with an illegal BAC, a law enforcement officer can charge you
with DUI. Even if your BAC is below legal limits, that does not mean it is
safe for you to drive. Almost everyone feels negative effects of alcohol,
even at levels lower than the legal limit. Depending on how badly you are
impaired, you may be arrested and convicted of a DUI even without a
BAC measurement.
The table below shows BAC estimates based on how many drinks are
consumed, gender, and body weight. Remember even one drink can
affect your ability to drive safely.
,
BLOOD ALCOHOL CONCENTRATION (BAC)
Table for Male (M) / Female (F)
Number of
Drinks
Body Weight in Pounds
Driving
Condition100 120 140 160 180 200 220 240
0
M .00 .00 .00 .00 .00 .00 .00 .00
Only Safe Driving
Limit
F .00 .00 .00 .00 .00 .00 .00 .00
1
M .06 .05 .04 .04 .03 .03 .03 .02
Driving Skills
Impaired
F .07 .06 .05 .04 .04 .03 .03 .03
2
M .12 .10 .09 .07 .07 .06 .05 .05
F .13 .11 .09 .08 .07 .07 .06 .06
3
M .18 .15 .13 .11 .10 .09 .08 .07
F .20 .17 .14 .12 .11 .10 .09 .08
Legally
Intoxicated
4
M .24 .20 .17 .15 .13 .12 .11 .10
F .26 .22 .19 .17 .15 .13 .12 .11
5
M .30 .25 .21 .19 .17 .15 .14 .12
F .33 .28 .24 .21 .18 .17 .15 .14
Subtract 0.01% for each 40 minutes that lapse between drinks.
1 drink = 1.5 oz. 80 proof liquor, 12 oz. 5% beer, or 5 oz. 12% wine.
Fewer than 5 persons out of 100 will exceed these values.
NOTE It is illegal to drink alcohol or take drugs when you are operating
a boat, jet ski, water skis, aquaplane, or similar vessels. Learn more in the
California Harbors and Navigation Code.

74
DUI A
When you drive in California, you consent to a breath, blood, or urine
test if a law enforcement officer suspects you of DUI. If you agreed to
take a preliminary alcohol screening (PAS) or breath test, you may still be
required to take a blood or urine test to detect the presence of drugs. If
you refuse, DMV will suspend or revoke your driving privilege. If you are
arrested for DUI:
• California’s Administrative Per Se law requires DMV to suspend your
driving privilege.
• The law enforcement officer may take your driver’s license and give
you a temporary driver’s license for 30 days.
• You may request a DMV administrative hearing within 10 days from
the date of your arrest.
DUI C
If you are convicted of a DUI, DMV will suspend or revoke your driving
privilege for one year. And you:
• Must complete a DUI program.
• Must le a California Insurance Proof Certicate (SR 22/SR 1P).
• Must pay any applicable license reissue or restriction fees.
• May be required to install an ignition interlock device (IID) on your
vehicle.
Here are some additional penalties if you are convicted of DUI:
• You may be sentenced to up to six months in jail.
• You may have to pay a ne.
• Law enforcement may impound your vehicle and you may have to
pay a storage fee.
• If you cause serious injury or death while driving under the inuence
of drugs or alcohol, you may face civil lawsuits.
All DUI convictions remain on your driver’s record for 10 years. If you
get any other DUIs during that time, the court or DMV may give you an
additional penalty.

75
D U 21
If you are under 21 years old, there are additional laws for possessing and
consuming alcohol.
Possessing alcohol:
• You may not carry any alcohol beverage inside a vehicle unless an
individual who is 21 years old or older is with you. The container must
be full, sealed, and unopened. If opened, the alcohol must be kept in
the trunk or place where passengers do not sit.
EXCEPTION: If you are working for someone with an off-site liquor
sales license, you may carry alcoholic beverages in closed containers.
• If you are caught with alcohol in your vehicle, law enforcement can
impound your vehicle for up to 30 days. The court may ne you and
suspend your driver’s license for one year. If you do not already have
a driver’s license, the court may ask DMV to delay giving you your rst
driver’s license for up to one year.
Consuming alcohol:
• If a law enforcement officer suspects you of consuming alcohol,
they can require you to take a hand-held breath test, PAS, or another
chemical test.
• If you are convicted of a DUI with a BAC of 0.01% or higher, DMV may
revoke your driving privilege for one year. You must also complete a
licensed DUI program.
• If your PAS shows a BAC of 0.05% or higher, the officer may require
you to take a breath or blood test.
• If a later test shows you have a BAC of 0.05% or higher, you may be
arrested for a DUI and your driving privilege may be suspended.

76
SECTION 10. Financial Responsibility, Insurance
Requirements, and Collisions
You must have your proof of nancial responsibility (insurance) when you
drive and for a drive test. If you get into a collision, you must show proof
to the other drivers involved in the collision.
I R
Your insurance must cover at least:
• $15,000 for a single death or injury.
• $30,000 for death or injury to more than one person.
• $5,000 for property damage.
Parents or guardians take on nancial responsibility for drivers younger
than 18 years old and pay for damages if the driver is involved in a
collision. Drivers who are 18 years old and older take on their own
nancial responsibility.
Before you buy insurance, make sure that the agent, broker, or insurance
provider is licensed by the California Department of Insurance. For more
information, visit insurance.ca.gov/license-status/.
Low-cost Insurance
If you cannot afford liability insurance, you may be eligible for the
California Low Cost Automobile Insurance Program. For more
information, visit mylowcostauto.com or call 1-866-602-8861.

77
C
Understand factors that lead to collisions so you can try to avoid them.
Causes of Collisions
The most common causes of collisions are:
• Driver distractions.
• Unsafe speed.
• Improper turns.
• Not following the right-of-way rules.
• Not following stop signals and signs.
• Driving on the wrong side of the road.
• A vehicle traveling faster or slower than the ow of traffic.
If you see a vehicle’s emergency ashers ahead, slow down. There may
be a collision or other road emergency. Pass carefully.
Avoid driving near collisions, if possible. If anyone is injured, they will get
help faster if other vehicles are not blocking the road.
What to Do if You Are in a Collision
If you are in a collision:
• You must stop. Someone could be injured and need your help. Failing
to stop or leaving the scene of an accident is called a hit-and-run.
The punishment is severe if you are convicted of a hit-and-run.
• Call 911 right away if anyone is hurt.
• Move your vehicle out of traffic if no one is hurt. Then call 911.
• Show your driver’s license, vehicle registration card, insurance
information, and current address to the other driver, law enforcement
officer, and anyone else involved in the collision.
• You must make a report to law enforcement within 24 hours of the
collision if anyone is injured or killed. Your insurance agent, broker, or
legal representative can also le the report.
• Try to nd the owner if your vehicle hits or rolls into a parked car or
other property. If you cannot nd the owner, leave a note with your
name, phone number, and address. Securely attach the note to the
vehicle or property. Report the collision to law enforcement.
• If you kill or injure an animal, call the nearest humane society or law
enforcement. Do not try to move an injured animal.

78
Reporting a Collision
If you are in a collision, you must report it to DMV within 10 days if:
• The collision caused more than $1,000 in damage to property.
• Anyone was injured or killed. This applies even if the injuries were
minor.
Each driver must le a Report of Traffic Accident Occurring in
California (SR 1) with DMV at dmv.ca.gov/accidentreport. You (or
your representative) must le a report whether or not you caused the
collision. This applies even if the collision happened on private property.
Your driving privilege will be suspended if you fail to le a report. Law
enforcement will not make a report for you.
Driving Without Insurance
Your driving privilege will be suspended for up to four years if you are in a
collision and do not have proper insurance coverage. It does not matter
who was at fault.
You can get your driver’s license back during the last three years of
the suspension if you provide a California Insurance Proof Certicate
(SR 22/SR 1P) and maintain it during the three-year period.
C Y D’ R
If you are involved in a collision resulting in $1,000 in damage, or where
anyone is injured or dies, it is your responsibility to report the collision
to DMV. DMV will add it to your driver’s record. It does not matter who
caused the collision.

79
SECTION 11. Vehicle Registration Requirements
You need to register your vehicle in California to use it in the state. For
more information, visit dmv.ca.gov/vrservices.
B S V
When you buy a vehicle, you have 10 days to transfer ownership to your
name.
When you sell a vehicle, you must notify DMV within ve days
by completing a Notice of Transfer and Release of Liability at
dmv.ca.gov/nrl.
O--S V
You have 20 days to register your vehicle after you become
a resident or get a job in California. For more information, visit
dmv.ca.gov/outofstatevr.
All vehicles registered in California are required to meet California
requirements including vehicle emission controls in support of
California’s clean air standards. DMV cannot register a vehicle if it does
not qualify.

80
SECTION 12. Driver Safety
Eventually, every driver will need to evaluate and assess their driving skills
and abilities. If you are concerned about your driving, ask a trusted driver
with a valid driver’s license to sit in the passenger seat and observe your
driving. Your observer should note any dangerous driving behaviors and
give suggestions for improvement. Listen carefully and apply what you
have learned. Consider professional driving lessons or driving classes as
an alternative.
Reexamination
The Vehicle Code allows DMV to investigate and reexamine every driver’s
ability to operate a motor vehicle safely. A physical or mental condition
or poor driver’s record can be the basis for a reexamination, not a driver’s
age. Drivers with a physical or mental condition can be referred to DMV
by a physician, law enforcement, or family member by submitting a
completed Request for Driver Reexamination form.
Cognitive disorders, such as dementia, seizure disorder, brain tumor,
Parkinson’s disease, stroke, or vertigo, present a signicant challenge to
safe driving. Individuals suffering from these conditions may lose their
ability to drive safely.
NOTE: When a referral or diagnosis for someone with a mild cognitive
impairment is received by DMV, the Driver Safety team will schedule
a reexamination. For more information regarding the reexamination
process, visit dmv.ca.gov/reexamination.
DMV may do the following:
• Request medical information from you or your physician.
• Conduct an in-person or over the telephone reexamination.
• Require you to take a knowledge, vision, or driving test(s).
• Issue you a limited term driver’s license.
• Immediately suspend or revoke your driving privilege if your physical
or mental condition presents an immediate threat to public safety.
• Take no action against your driving privilege.

81
Priority Reexamination
If you come in contact with law enforcement and receive a Notice
of Priority Reexamination of Driver with a check mark in the top box
carefully read the form. You have ve working days to contact DMV
to initiate the process or your driving privilege will be automatically
suspended.
REQUEST FOR REGULAR RE-EXAMINATION OF DRIVER (Ocer’s Instructions on reverse.)
The driver listed below should be re-examined by DMV, but does not require a Priority Re-examination.
OBSERVED DRIVING BEHAVIOR—Check appropriate boxes for driving problems you observed: (Use space below if needed for additional comments.)
DATE TIME DRIVER LICENSE NO. STATE BIRTHDATE
NAME (FIRST, MIDDLE, LAST)
MAILING ADDRESS
CITY STATE ZIP CODE DRIVER’S DAYTIME PHONE NO.
LOCATION OF INCIDENT
ANY NOTICE TO APPEAR NO. (IF CITATION ISSUED, ATTACH COPY)
ACCIDENT/ARREST NO. (ATTACH COPY IF APPLICABLE) CITY COUNTY
FOR DMV USE ONLY
X - ( )
NOTICE OF PRIORITY RE-EXAMINATION OF DRIVER (Driver Incapacity)
The driver listed below committed a violation of the California Vehicle Code (CVC) §§21000 through 23336 and should be
re-examined pursuant to CVC §21061. At the time of the violation, the driver exhibited evidence of incapacity which reasonably
led me to believe that this person is not capable of operating a motor vehicle without presenting a clear or potential danger, or
risk of injury to himself/herself or others. As required by law, on the date below, I issued a copy of this Notice of Priority
Re-examination/Notice of Suspension for Non-Compliance to the driver listed below.
The driver does not have to be cited for one of the above CVC sections. Please indicate evidence of the incapacity in the
Summary area below. If the driver was involved in a trac accident, attach a copy of the report. You must give a copy of
this form to the driver.
If this form is being issued as a Notice of Priority Re-examination/Notice of Suspension for Non-Compliance, immediately
fax the document (if fax available) to the Driver Safety Oce nearest the driver’s home (see reverse), then mail the original
Notice to the same oce.
NOTICE OF SUSPENSION FOR NON-COMPLIANCE
INSTRUCTIONS TO DRIVER
If the above box is checked, you must contact the Department of Motor Vehicles (DMV) for a re-examination under CVC §§12818
and 12819. If you do not call or appear within ve (5) working days, your privilege to drive in this state will be suspended until you
satisfactorily complete a re-examination. SEE IMPORTANT PRIORITY RE-EXAMINATION INFORMATION ON THE REVERSE
SIDE OF THIS FORM.
DS 427 (REV. 10/2018)
Yes No
( )
AGENCY TELEPHONE NO.
STREET ADDRESS CITY ZIP CODE
OFFICER NAME (PLEASE PRINT) BADGE OR I.D. NUMBER
OFFICER’S SIGNATURE DATE DATE FAXED DO YOU WISH TO BE NOTIFIED OF RESULTS?
I certify (or declare) under penalty of perjury under the laws of the State of California that the information I have
provided is true and correct.
X
SUMMARY: You may use the space below to further describe actions of the driver which led you to believe a re-examination
is needed - describe any impairment, serious physical injury or illness, mental impairment or disorientation. Describe any
trac law violations whether or not a citation was issued.
Confused, disoriented, incoherent, or unaware of actions
Reported/Observed Medical Condition
Little or no recollection of incident
Medicated
Vision Condition/Visual Impairment
Mental/Emotional Condition
Driver reported he/she did not see cars, pedestrians, etc.
Diculty Walking
Weakness or Coordination Problems
Responding incorrectly to Emergency Signal/Lights
Drifting or weaving in and out of lanes
Caused, or nearly caused, collision
Not reacting to other cars, pedestrians, etc.
Driving on wrong side of road
Driving on sidewalk
Driving in wrong lane
Driving too slow, impeding trac
Failed to stop at red light/stop sign
Unsafe/inappropriate lane change
Inappropriately stopped
Failed to yield right-of-way
Lost control of vehicle
Struck stationary object
Failed to go on green light
Driving without lights during darkness
Made turn from wrong lane
Fell asleep while driving
Violent or aggressive driving
Not adequately controlling vehicle
Other Observations _________________________________________
____________________________________________________________
DRIVER CONDITION (Observations after Stop/Collision)—Check all appropriate boxes below. Please use the space below to provide specic
details, if known, and the driver’s medical (physical or mental) condition such as name of disease or illness, any medications taken, etc.
Alcohol/Drug Use (Describe below)
Confused by trac
Lost or confused while driving near home
Blackout/Seizure/Fainting
Driver appears to need help with hygiene
and/or dressing appropriately
Other Observations _________________________________________
____________________________________________________________
Destroy all previous versions of this form.
White: DMV Canary: Law Enforcement Pink: Driver (Priority Re-Exam Only)
,
Driver’s License Restrictions
DMV places restrictions on a driver’s license to ensure a driver is
operating a vehicle within their ability. Restrictions may be imposed by
DMV or required by law. Restrictions placed on your driving privilege will
be reasonable and necessary for your safety and the safety of others.
Restrictions and conditions may include:
• Requiring a driver to place special mechanical devices on their
vehicle, such as hand controls.
• Limiting when and where a person may drive, such as no night or
freeway driving.
• Requiring eyeglasses or corrective contact lenses.
• Requiring additional devices, such as outside mirrors.
NOTE: There are no specic restrictions for seniors. All restrictions are
based on conditions, not age.
Any restriction placed on your driver’s license is based on the examiner’s
ndings and recommendations.

82
SECTION 13. Seniors and Driving
Senior drivers often have unique needs and concerns about driving.
Driving requires certain physical, visual, and mental abilities. We all want
to continue driving as long as we can. However, the time may come when
we must limit or stop driving temporarily or permanently. Here are some
warning signs of an unsafe driver:
• Getting lost in familiar places.
• Dents and scrapes on the car, fences, mailbox, garage doors, etc.
• Frequent close calls or collisions.
Senior drivers may consider:
• Limiting or not driving at night.
— If night driving is necessary, choose a well-lit route.
• Driving during the time of day when traffic is light.
• Avoiding difficult intersections.
• Driving for short distances or limiting driving to essential places.
• No freeway driving.
• Installing an additional right-side mirror.
To get the Driver Skills Self-Assessment Questionnaire, visit
dmv.ca.gov/driver-skills.
Driver’s License Renewal
If you are 70 years old or older at the time your driver’s license expires,
you are required to renew your driver’s license in person, unless
otherwise instructed by DMV. Knowledge and vision tests are required.
If you do not pass, you may be issued a temporary driver’s license.
DMV sends a renewal notice to your address of record about 60 days
before your driver’s license expires. If you do not receive a renewal
notice, complete a Driver License or Identication Card Application at
dmv.ca.gov/dlservices or at a DMV office. Visit dmv.ca.gov/driver-ed for
more information and sample tests.
DMV’s Community Liaison and Outreach
The Community Liaison’s primary function is to represent public safety
interests for all Californians, with a focus in addressing the concerns
of senior drivers and teens. The liaison can assist as a go-between to
ensure drivers are treated fairly, consistently with laws and regulations,

83
and with dignity and respect. While the Community Liaison cannot
represent you in a DMV hearing or reexamination, they can provide you
with useful tools and information.
For information about outreach services in your area or to speak to a
liaison, contact Community Liaison and Outreach at (833) 493-0675.
Cognitive Impairment
Seniors suffering from dementia present a signicant challenge to
safe driving. Individuals with progressive dementia ultimately lose their
ability to drive safely. It is often up to caregivers, physicians, and law
enforcement, to stop these seniors from driving and arrange alternative
transportation. For more information about the reexamination process,
visit dmv.ca.gov/reexamination.
Mature Driver Program
The Mature Driver Improvement Program is an eight-hour course for
drivers 55 years old and older. It covers a range of topics that are of
special interest to mature drivers.
Your insurance company may offer discounts if you complete the
program. Contact your insurance provider with a copy of your
completion certicate. Your certicate is valid for three years. You can
renew it by completing another four-hour course.
You can take the course through DMV-approved providers. Visit
dmv.ca.gov/seniors for more information, including locations near you.
Senior ID Cards
If you are 62 years old or older, you are eligible for a no-fee Senior ID
card. Drivers of any age who are unable to continue driving safely due to
a physical or mental condition may be eligible to exchange their driver’s
license for a no-fee ID card. The ID card serves as identication only.
Details may be found at dmv.ca.gov/id-cards.

84
SECTION 14 Glossary.
TERM DEFINITION
Behind-the-
wheel drive
test
A drive test where you have control of the vehicle and are
accompanied by a DMV examiner who is evaluating your
driving skills.
Blood alcohol
concentration
(BAC)
Your BAC is the amount of alcohol in your blood. For
example, if your BAC is 0.10%, that means you have 0.10
grams of alcohol in 100 milliliters of blood.
Driving
performance
evaluation
(DPE)
DPE is the portion of the behind-the-wheel drive test
when you drive your car with a DMV examiner who
evaluates your driving skills.
Pedestrian A pedestrian can also be a person with a disability using a
tricycle, quadricycle, or wheelchair for transportation.
Right-of-way
Helps determine who is allowed to go rst in situations
where vehicles, pedestrians, and cyclists meet on the
road.
Three-second
rule
A driving rule that helps you estimate how closely you
should follow other vehicles. When the vehicle in front of
you passes a certain point, such as a sign, count three
seconds. If you pass the same point before you nish
counting, you are following too closely.
Traffic citation Also known as a ticket, a traffic citation is an official
summons issued by law enforcement for violating a traffic
law.
Vulnerable
road users
(VRU)
VRUs are non-motorized road users, such as cyclists,
pedestrians, and persons with disabilities or reduced
mobility and orientation using a wheelchair, tricycle, or
quadricycle.
Yield
Yield means to wait for, slow down, and be ready to stop
(if necessary) to allow other vehicles or pedestrians who
have right-of-way to proceed.
Use your computer, tablet,
or smartphone to ll out the
online renewal application
before visiting a DMV office.
Save Time
GO ONLINE to ll out
your driver’s license or ID
renewal application
Available in 10 languages
English Spanish
Chinese Japanese
Korean Tagalog
Thai Vietnamese
Hindi Khmer

Use
your
computer, tablet,
or smartphone
to
fill
out
the
online renewal application
before visiting a DMV office.
Available
in
10
languages
English Spanish
Chinese Japanese
Korean Tagalog
Thai Vietnamese
Hindi Khmer
STATE
OF
CALIFORNIA
~--~•=
RttV&-
Department
of
Motor Vehicles.

Opt-in for paperless notices
for your driver’s license, ID card,
or vehicle registration.
GO
PAPERLESS!
Make your selection at
dmv.ca.gov/paperless
.Reduce, reuse, recycle this handbook
