

2
TableofContents
Cocaine
Whatiscocaine?
WhatisthescopeofcocaineuseintheUnitedStates?
Howiscocaineused?
Howdoescocaineproduceitseffects?
Whataresomewaysthatcocainechangesthebrain?
Whataretheshort-termeffectsofcocaineuse?
Whatarethelong-termeffectsofcocaineuse?
WhyarecocaineusersatriskforcontractingHIV/AIDSandhepatitis?
Whataretheeffectsofmaternalcocaineuse?
Howiscocaineaddictiontreated?
Howiscutting-edgesciencehelpingusbetterunderstandaddiction?
References
WherecanIgetfurtherinformationaboutcocaine?

3
Whatiscocaine?
Cocaineisapowerfullyaddictivestimulantdrug.Forthousandsof
years,peopleinSouthAmericahavechewedandingestedcocaleaves
(Erythroxyloncoca),thesourceofcocaine,fortheirstimulant
effects. Thepurifiedchemical,cocainehydrochloride,wasisolated
fromtheplantmorethan100yearsago.Intheearly1900s,purified
cocainewasthemainactiveingredientinmanytonicsandelixirs
developedtotreatawidevarietyofillnessesandwasevenan
ingredientintheearlyformulationsofCoca-Cola .Beforethe
developmentofsyntheticlocalanesthetic,surgeonsusedcocaineto
blockpain. However,researchhassinceshownthatcocaineisa
powerfullyaddictivesubstancethatcanalterbrainstructureand
functionifusedrepeatedly.
Today,cocaineisaScheduleIIdrug,whichmeansthatithashigh
potentialforabusebutcanbeadministeredbyadoctorforlegitimate
medicaluses,suchaslocalanesthesiaforsomeeye,ear,andthroat
surgeries.Asastreetdrug,cocaineappearsasafine,white,crystalline
powderandisalsoknownasCoke,C,Snow,Powder,orBlow.Street
dealersoftendilute(or“cut”)itwithnon-psychoactivesubstancessuch
ascornstarch,talcumpowder,flour,orbakingsodatoincreasetheir
profits.Theymayalsoadulteratecocainewithotherdrugslikeprocaine
Photoby©iStock.com/RafalCichawa
1,2
®
1

4
(achemicallyrelatedlocalanesthetic)oramphetamine(another
psychoactivestimulant). Someuserscombinecocainewithheroin—
calledaSpeedball.
Peopleabusetwochemicalformsofcocaine:thewater-soluble
hydrochloridesaltandthewater-insolublecocainebase(orfreebase).
Usersinjectorsnortthehydrochloridesalt,whichisapowder.The
baseformofcocaineiscreatedbyprocessingthedrugwithammonia
orsodiumbicarbonate(bakingsoda)andwater,thenheatingitto
removethehydrochloridetoproduceasmokablesubstance.Theterm
crack,whichisthestreetnamegiventofreebasecocaine,referstothe
cracklingsoundheardwhenthemixtureissmoked.
2,3
2
2

5
Whatisthescopeofcocaine
useintheUnitedStates?
AccordingtotheNationalSurveyonDrugUseandHealth(NSDUH),
cocaineusehasremainedrelativelystablesince2009.In2014,there
wereanestimated1.5millioncurrent(past-month)cocaineusersaged
12orolder(0.6percentofthepopulation).Adultsaged18to25years
haveahigherrateofcurrentcocaineusethananyotheragegroup,
with1.4percentofyoungadultsreportingpast-monthcocaineuse.
The2015MonitoringtheFuturesurvey,whichannuallysurveysteen
attitudesanddruguse,reportsasignificantdeclinein30-day
prevalenceofpowdercocaineuseamong8th,10th,and12thgraders
frompeakuseinthelate1990s.In2014,1.1percentof12thgraders
andonly0.8percentof10thandhalfapercentof8thgradersreported
usingcocaineinthepastmonth.
4
Source:UniversityofMichigan,MonitoringtheFuturenationalresultsondruguse:
1975-2015:overview,keyfindingsonadolescentdruguse,2016.
5

6
Repeatedcocaineusecanproduceaddictionandotheradversehealth
consequences.In2014,accordingtotheNSDUH,about913,000
AmericansmettheDiagnosticandStatisticalManualofMental
Disorderscriteriafordependenceorabuseofcocaine(inanyform)
duringthepast12months.Further,datafromthe2011DrugAbuse
WarningNetwork(DAWN)reportshowedthatcocainewasinvolvedin
505,224ofthenearly1.3millionvisitstoemergencydepartmentsfor
drugmisuseorabuse.Thistranslatestooveroneinthreedrugmisuse
orabuse-relatedemergencydepartmentvisits(40percent)that
involvedcocaine.
6

7
Howiscocaineused?
Usersprimarilyadministercocaineorally,intranasally,intravenously,
orbyinhalation.Whenpeoplesnortthedrug(intranasaluse),they
inhalecocainepowderthroughthenostrils,whereitisabsorbedinto
thebloodstreamthroughthenasaltissues.Usersalsomayrubthe
drugontotheirgums(oraluse).Dissolvingcocaineinwaterand
injectingit(intravenoususe)releasesthedrugdirectlyintothe
bloodstreamandheightenstheintensityofitseffects.Whenpeople
smokecocaine(inhalation),theyinhaleitsvapororsmokeintothe
lungs,whereabsorptionintothebloodstreamisalmostasrapidasby
injection.Thisfasteuphoriceffectisoneofthereasonsthatcrack
becameenormouslypopularinthemid-1980s.
PhotobyDEA/
Cocaine
2

8
Cocaineuserangesfromoccasionaltorepeatedorcompulsiveuse,
withavarietyofpatternsbetweentheseextremes.Anyrouteof
administrationcanpotentiallyleadtoabsorptionoftoxicamountsof
cocaine,causingheartattacks,strokes,orseizures—allofwhichcan
resultinsuddendeath.
PhotobyDEA/
Crackcocaine
2,7

9
Howdoescocaineproduceits
effects?
Thebrain’smesolimbicdopaminesystem,itsrewardpathway,is
stimulatedbyalltypesofreinforcingstimuli,suchasfood,sex,and
manydrugsofabuse,includingcocaine. Thispathwayoriginatesina
regionofthemidbraincalledtheventraltegmentalareaandextends
tothenucleusaccumbens,oneofthebrain’skeyrewardareas.
Besidesreward,thiscircuitalsoregulatesemotionsandmotivation.
Inthenormalcommunicationprocess,dopamineisreleasedbya
neuronintothesynapse(thesmallgapbetweentwoneurons),whereit
bindstospecializedproteinscalleddopaminereceptorsonthe
neighboringneuron.Bythisprocess,dopamineactsasachemical
messenger,carryingasignalfromneurontoneuron.Another
specializedproteincalledatransporterremovesdopaminefromthe
synapsetoberecycledforfurtheruse.
Drugsofabusecaninterferewiththisnormalcommunicationprocess.
Forexample,cocaineactsbybindingtothedopaminetransporter,
blockingtheremovalofdopaminefromthesynapse.Dopaminethen
accumulatesinthesynapsetoproduceanamplifiedsignaltothe
receivingneurons.Thisiswhatcausestheeuphoriacommonly
experiencedimmediatelyaftertakingthedrug(seethevideo"Brain
Reward:UnderstandingHowtheBrainRespondstoNaturalRewards
andDrugsofAbuse").
8
8
8

10
ImagebyNIDA
Cocaineinthebrain:Inthenormalneuralcommunicationprocess,
dopamineisreleasedbyaneuronintothesynapse,whereitcanbindto
dopaminereceptorsonneighboringneurons.Normally,dopamineisthen
recycledbackintothetransmittingneuronbyaspecializedproteincalled
thedopaminetransporter.Ifcocaineispresent,itattachestothe
dopaminetransporterandblocksthenormalrecyclingprocess,resultingin
abuildupofdopamineinthesynapse,whichcontributestothe
pleasurableeffectsofcocaine.

11
Whataresomewaysthat
cocainechangesthebrain?
Useofcocaine,likeotherdrugsofabuse,induceslong-termchangesin
thebrain.Animalstudiesshowthatcocaineexposurecancause
significantneuroadaptationsinneuronsthatreleasetheexcitatory
neurotransmitterglutamate. Animalschronicallyexposedtococaine
demonstrateprofoundchangesinglutamateneurotransmission—
includinghowmuchisreleasedandthelevelofreceptorproteins—in
therewardpathway,particularlythenucleusaccumbens.The
glutamatesystemmaybeanopportunetargetforanti-addiction
medicationdevelopment,withthegoalofreversingthecocaine-
inducedneuroadaptationsthatcontributetothedrivetousethedrug.
Althoughaddictionresearchershavefocusedonadaptationsinthe
brain’srewardsystem,drugsalsoaffectthebrainpathwaysthat
respondtostress.Stresscancontributetococainerelapse,and
cocaineusedisordersfrequentlyco-occurwithstress-related
disorders. Thestresscircuitsofthebrainaredistinctfromthereward
pathway,butresearchindicatesthatthereareimportantwaysthat
theyoverlap.Theventraltegmentalareaseemstoactasacritical
integrationsiteinthebrainthatrelaysinformationaboutbothstress
anddrugcuestootherareasofthebrain,includingonesthatdrive
cocaineseeking. Animalsthathavereceivedcocainerepeatedlyare
morelikelytoseekthedruginresponsetostress,andthemoreofthe
drugtheyhavetaken,themorestressaffectsthisbehavior. Research
suggeststhatcocaineelevatesstresshormones,inducing
neuroadaptationsthatfurtherincreasesensitivitytothedrugandcues
associatedwithit.
9,10
9
11
11
11
11

12
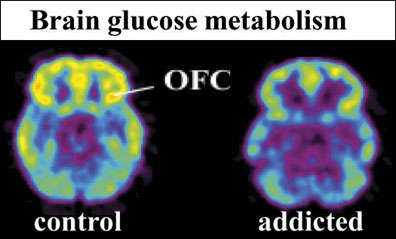
Chroniccocaineexposureaffectsmanyotherareasofthebraintoo.For
example,animalresearchindicatesthatcocainediminishesfunctioning
intheorbitofrontalcortex(OFC),whichappearstounderliethepoor
decision-making,inabilitytoadapttonegativeconsequencesofdrug
use,andlackofself-insightshownbypeopleaddictedtococaine. A
studyusingoptogenetictechnology,whichuseslighttoactivate
specific,genetically-modifiedneurons,foundthatstimulatingtheOFC
restoresadaptivelearninginanimals.Thisintriguingresultsuggests
thatstrengtheningOFCactivitymaybeagoodtherapeuticapproachto
improveinsightandawarenessoftheconsequencesofdruguse
amongpeopleaddictedtococaine.
Brainimagesshowingdecreasedglucosemetabolism,whichindicates
reducedactivity,intheorbitofrontalcortex(OFC)inacontrolsubject(left)
andacocaine-addictedsubject(right).
VolkowND,WantG-J,FowlerJS,TomasiD,TelandF.Addiction:beyond
dopaminerewardcircuitry.ProcNatlAcadSciUSA.2011;108(37):15037-
15042.
12
13

13
Whataretheshort-term
effectsofcocaineuse?
Cocaine’seffectsappearalmostimmediatelyafterasingledoseand
disappearwithinafewminutestoanhour.Smallamountsofcocaine
usuallymaketheuserfeeleuphoric,energetic,talkative,mentally
alert,andhypersensitivetosight,sound,andtouch.Thedrugcanalso
temporarilydecreasetheneedforfoodandsleep. Someusersfind
thatcocainehelpsthemperformsimplephysicalandintellectualtasks
morequickly,althoughothersexperiencetheoppositeeffect.
Thedurationofcocaine’seuphoriceffectsdependupontherouteof
administration.Thefasterthedrugisabsorbed,themoreintensethe
resultinghigh,butalsotheshorteritsduration.Snortingcocaine
producesarelativelyslowonsetofthehigh,butitmaylastfrom15to
30minutes.Incontrast,thehighfromsmokingismoreimmediatebut
maylastonly5to10minutes.
Short-termphysiologicaleffectsofcocaineuseincludeconstricted
bloodvessels;dilatedpupils;andincreasedbodytemperature,heart
rate,andbloodpressure. Largeamountsofcocainemayintensifythe
user’shighbutcanalsoleadtobizarre,erratic,andviolentbehavior.
Somecocaineusersreportfeelingsofrestlessness,irritability,anxiety,
panic,andparanoia. Usersmayalsoexperiencetremors,vertigo,and
muscletwitches.
Severemedicalcomplicationscanoccurwithcocaineuse.Someofthe
mostfrequentarecardiovasculareffects,includingdisturbancesin
heartrhythmandheartattacks;neurologicaleffects,including
headaches,seizures,strokes,andcoma;andgastrointestinal
complications,includingabdominalpainandnausea. Inrare
instances,suddendeathcanoccuronthefirstuseofcocaineor
unexpectedlythereafter.Cocaine-relateddeathsareoftenaresultof
cardiacarrestorseizures (see"NationalOverdoseDeaths:Numberof
DeathsfromCocaine").Manycocaineusersalsousealcohol,andthis
14
15
16
2
2
7
2

14
combinationcanbeparticularlydangerous.Thetwosubstancesreact
toproducecocaethylene,whichmaypotentiatethetoxiceffectsof
cocaineandalcoholontheheart. Thecombinationofcocaineand
heroinisalsoverydangerous.Userscombinethesedrugsbecausethe
stimulatingeffectsofcocaineareoffsetbythesedatingeffectsof
heroin;however,thiscanleadtotakingahighdoseofheroinwithout
initiallyrealizingit.Becausecocaine'seffectswearoffsooner,thiscan
leadtoaheroinoverdose,inwhichtheuser'srespirationdangerously
slowsdownorstops,possiblyfatally.
17

15
Whatarethelong-termeffects
ofcocaineuse?
Withrepeatedexposuretococaine,thebrainstartstoadaptsothat
therewardpathwaybecomeslesssensitivetonaturalreinforcers
(see"WhatAreSomeWaysthatCocaineChangestheBrain?").Atthe
sametime,circuitsinvolvedinstressbecomeincreasinglysensitive,
leadingtoincreaseddispleasureandnegativemoodswhennottaking
thedrug,whicharesignsofwithdrawal.Thesecombinedeffectsmake
theusermorelikelytofocusonseekingthedruginsteadof
relationships,food,orothernaturalrewards.
Withregularuse,tolerancemaydevelopsothathigherdoses,more
frequentuseofcocaine,orbothareneededtoproducethesamelevel
ofpleasureandrelieffromwithdrawalexperiencedinitially. Atthe
sametime,userscanalsodevelopsensitization,inwhichlesscocaine
isneededtoproduceanxiety,convulsions,orothertoxiceffects.
Tolerancetococainerewardandsensitizationtococainetoxicitycan
increasetheriskofoverdoseinaregularuser.
Userstakecocaineinbinges,inwhichcocaineisusedrepeatedlyand
atincreasinglyhigherdoses.Thiscanleadtoincreasedirritability,
restlessness,panicattacks,paranoia,andevenafull-blownpsychosis,
inwhichtheindividuallosestouchwithrealityandexperiences
auditoryhallucinations. Withincreasingdosesorhigherfrequencyof
use,theriskofadversepsychologicalorphysiologicaleffects
increases. Animalresearchsuggeststhatbingingoncocaineduring
adolescenceenhancessensitivitytotherewardingeffectsofcocaine
andMDMA(EcstasyorMolly). Thus,bingeuseofcocaineduring
adolescencemayfurtherincreasevulnerabilitytocontinueduseofthe
drugamongsomepeople.
Specificroutesofcocaineadministrationcanproducetheirown
adverseeffects.Regularlysnortingcocainecanleadtolossofsenseof
smell,nosebleeds,problemswithswallowing,hoarseness,andan
10,18
10,18
7
2
2,7
19

16
overallirritationofthenasalseptumleadingtoachronicallyinflamed,
runnynose. Smokingcrackcocainedamagesthelungsandcan
worsenasthma. Peoplewhoinjectcocainehavepuncturemarks
calledtracks,mostcommonlyintheirforearms, andtheyareatriskof
contractinginfectiousdiseaseslikeHIVandhepatitisC(see"WhyAre
CocaineUsersatRiskforContractingHIVandHepatitis?").Theyalso
mayexperienceallergicreactions,eithertothedrugitselforto
additivesinstreetcocaine,whichinseverecasescanresultindeath.
Cocainedamagesmanyotherorgansinthebody.Itreducesbloodflow
inthegastrointestinaltract,whichcanleadtotearsandulcerations.
Manychroniccocaineuserslosetheirappetiteandexperience
significantweightlossandmalnourishment.Cocainehassignificant
andwell-recognizedtoxiceffectsontheheartandcardiovascular
system. Chestpainthatfeelslikeaheartattackiscommonand
sendsmanycocaineuserstotheemergencyroom. Cocaineuseis
linkedwithincreasedriskofstroke, aswellasinflammationofthe
heartmuscle,deteriorationoftheabilityofthehearttocontract,and
aorticruptures.
Inadditiontotheincreasedriskforstrokeandseizures,other
neurologicalproblemscanoccurwithlong-termcocaineuse. There
havebeenreportsofintracerebralhemorrhage,orbleedingwithinthe
brain,andballoon-likebulgesinthewallsofcerebralbloodvessels.
Movementdisorders,includingParkinson’sdisease,mayalsooccur
aftermanyyearsofcocaineuse. Generally,studiessuggestthata
widerangeofcognitivefunctionsareimpairedwithlong-termcocaine
use—suchassustainingattention,impulseinhibition,memory,making
decisionsinvolvingrewardsorpunishments,andperformingmotor
tasks.
Formercocaineusersareathighriskforrelapse,evenfollowinglong
periodsofabstinence.Researchindicatesthatduringperiodsof
abstinence,thememoryofthecocaineexperienceorexposuretocues
associatedwithdrugusecantriggerstrongcravings,whichcanleadto
relapse.
15
2,3
7
7
7,16,20
7,20
16
20
7,18
7,18
7
14
21

17
Whyarecocaineusersatrisk
forcontractingHIV/AIDSand
hepatitis?
Drugintoxicationandaddictioncancompromisejudgmentand
decision-makingandpotentiallyleadtoriskysexualbehavior,including
tradingsexfordrugs,andneedlesharing.Thisincreasesacocaine
user’sriskforcontractinginfectiousdiseasessuchasHIVandhepatitis
C(HCV). TherearenovaccinestopreventHIVorHCVinfections.
StudiesthatexaminepatternsofHIVinfectionandprogressionhave
demonstratedthatcocaineuseacceleratesHIVinfection. Research
indicatesthatcocaineimpairsimmunecellfunction, promotes
replicationoftheHIVvirus,andpotentiatesthedamagingeffectsof
HIVondifferenttypesofcellsinthebrainandspinalcord,resultingin
furtherdamage. Studiesalsosuggestthatcocaineuseaccelerates
thedevelopmentofNeuroAIDS,neurologicalconditionsassociatedwith
HIVinfection.SymptomsofNeuroAIDSincludememoryloss,
movementproblems,andvisionimpairment.
CocaineuserswithHIVoftenhaveadvancedprogressionofthe
disease,withincreasedviralloadandaccelerateddecreasesinCD4+
cellcounts.InfectionwithHIVincreasesriskforco-infectionwithHCV,
avirusthataffectstheliver. Co-infectioncanleadtoseriousillnesses
—includingproblemswiththeimmunesystemandneurologic
conditions.Livercomplicationsareverycommon,withmanyco-
infectedindividualsdyingofchronicliverdiseaseandcancer.
AlthoughthelinkbetweeninjectiondruguseandHIV/HCViswell
established,morestudiesareneededtounderstandthemolecular
mechanismsunderlyingthisincreasedriskofco-infectioninnon-
injectingsubstanceusers.
Theinteractionofsubstanceuse,HIV,andhepatitismayaccelerate
diseaseprogression.Forexample,HIVspeedsthecourseofHCV
22
23
24
23
23
24
22
24

18
infectionbyacceleratingtheprogressionofhepatitis-associatedliver
disease. ResearchhaslinkedHIV/HCVco-infectionwithincreased
mortalitywhencomparedtoeitherinfectionalone. Substanceuse
andco-infectionlikelynegativelyinfluenceHIVdiseaseprogressionand
theabilityofthebodytomarshalanimmuneresponse.
PatientswithHIV/HCVco-infectioncanbenefitfromsubstanceabuse
treatmentandantiretroviraltherapies,whenclosely
monitored. Antiretroviraltreatmentisnoteffectiveforeveryoneand
canhavesignificantsideeffects,necessitatingclosemedical
supervision.TestingforHIVandHCVisrecommendedforanyindividual
whohaseverinjecteddrugs,sincethediseaseishighlytransmissible
viainjection.
24
24
24
22

19
Whataretheeffectsof
maternalcocaineuse?
Mostwomenwhoareaddictedtococaineareofchildbearingage.
Estimatessuggestthatabout5percentofpregnantwomenuseoneor
moreaddictivesubstances, andtherearearound750,000cocaine-
exposedpregnancieseveryyear. Althoughwomenmaybereluctant
toreportsubstanceusepatternsbecauseofsocialstigmaandfearof
losingcustodyoftheirchildren,theyshouldbeawarethatdruguse
whilepregnantisassociatedwithspecificrisksthatmaybereduced
withappropriatecare.
Cocaineuseduringpregnancyisassociatedwithmaternalmigraines
andseizures,prematuremembranerupture,andseparationofthe
placentalliningfromtheuteruspriortodelivery. Pregnancyis
accompaniedbynormalcardiovascularchanges,andcocaineuse
exacerbatesthese—sometimesleadingtoseriousproblemswithhigh
bloodpressure(hypertensivecrises),spontaneousmiscarriage,
pretermlabor,anddifficultdelivery. Cocaine-usingpregnantwomen
mustreceiveappropriatemedicalandpsychologicalcare—including
addictiontreatment—toreducetheserisks.
Sex-specificaddictiontreatmentandcomprehensiveservices—
includingprenatalcare,mentalhealthcounseling,
vocational/employmentassistance,andparentingskillstraining—can
promotedrugabstinenceandotherpositivehealthbehaviors.
Motivationalincentives/contingencymanagement(see"Behavioral
Interventions")asanadjuncttootheraddictiontreatmentisa
particularlypromisingstrategytoengagewomeninprenatalcareand
counselingforsubstanceuse.
Itisdifficulttoestimatethefullextentoftheconsequencesof
maternaldruguseandtodeterminethespecifichazardofaparticular
drugtotheunbornchild.Thisisbecausemultiplefactors—suchasthe
amountandnumberofalldrugsused,includingnicotineoralcohol;
25
26
25
26
25
27
28

20
extentofprenatalcare;exposuretoviolenceintheenvironment;
socioeconomicconditions;maternalnutrition;otherhealthconditions;
andexposuretosexuallytransmitteddiseases—canallinteractto
influencematernalandchildoutcomes. Similarly,parenting
styles,qualityofcareduringearlychildhood,exposuretoviolence,and
continuedparentaldrugusearestrongenvironmentalfactors
influencingoutcomes.
Babiesborntomotherswhousecocaineduringpregnancyareoften
prematurelydelivered,havelowbirthweightsandsmallerhead
circumferences,andareshorterinlengththanbabiesborntomothers
whodonotusecocaine. Direpredictionsofreducedintelligence
andsocialskillsinbabiesborntomotherswhousedcrackcocaine
whilepregnantduringthe1980s—so-called"crackbabies"—were
grosslyexaggerated.However,thefactthatmostofthesechildrendo
notshowseriousovertdeficitsshouldnotbeoverinterpretedto
indicatethatthereisnocauseforconcern.
Usingsophisticatedtechnologies,scientistsarenowfindingthat
exposuretococaineduringfetaldevelopmentmayleadtosubtle,yet
significant,laterdeficitsinsomechildren. Theseincludebehavior
problems(e.g.,difficultieswithself-regulation)anddeficitsinsome
aspectsofcognitiveperformance,informationprocessing,and
sustainedattentiontotasks—abilitiesthatareimportantforthe
realizationofachild’sfullpotential. Somedeficitspersistintothe
lateryears,withprenatallyexposedadolescentsshowingincreased
riskforsubtleproblemswithlanguageandmemory. Brainscansin
teenssuggeststhatat-restfunctioningofsomebrainregions—
includingareasinvolvedinattention,planning,andlanguage—may
differfromthatofnon-exposedpeers. Moreresearchisneededon
thelong-termeffectsofprenatalcocaineexposure.
26,29,30
31,32
26,29,30
31,32
32,33
34
35

21
Howiscocaineaddiction
treated?
In2013,cocaineaccountedforalmost6percentofalladmissionsto
drugabusetreatmentprograms.Themajorityofindividuals(68
percentin2013)whoseektreatmentforcocaineusesmokecrackand
arelikelytobepolydrugusers,meaningtheyusemorethanone
substance. Thosewhoprovidetreatmentforcocaineuseshould
recognizethatdrugaddictionisacomplexdiseaseinvolvingchanges
inthebrainaswellasawiderangeofsocial,familial,andother
environmentalfactors;therefore,treatmentofcocaineaddictionmust
addressthisbroadcontextaswellasanyotherco-occurringmental
disordersthatrequireadditionalbehavioralorpharmacological
interventions.
PharmacologicalApproaches
Presently,therearenomedicationsapprovedbytheU.S.Foodand
DrugAdministrationtotreatcocaineaddiction,thoughresearchersare
exploringavarietyofneurobiologicaltargets.Pastresearchhas
primarilyfocusedondopamine,butscientistshavealsofoundthat
cocaineuseinduceschangesinthebrainrelatedtoother
neurotransmitters—includingserotonin,gamma-aminobutyricacid
(GABA),norepinephrine,andglutamate. Researchersarecurrently
testingmedicationsthatactatthedopamineD receptor,asubtypeof
dopaminereceptorthatisabundantintheemotionandrewardcenters
ofthebrain. Otherresearchistestingcompounds(e.g.,N-
acetylcysteine)thatrestorethebalancebetweenexcitatory
(glutamate)andinhibitory(GABA)neurotransmission,whichis
disruptedbylong-termcocaineuse. Researchinanimalsisalso
lookingatmedications(e.g.,lorcaserin)thatactatserotonin
receptors.
Severalmedicationsmarketedforotherdiseasesshowpromisein
reducingcocaineusewithincontrolledclinicaltrials.Amongthese,
36
37
3
38
39
40

22
disulfiram,whichisusedtotreatalcoholism,hasshownthemost
promise.Scientistsdonotyetknowexactlyhowdisulfiramreduces
cocaineuse,thoughitseffectsmayberelatedtoitsabilitytoinhibitan
enzymethatconvertsdopaminetonorepinephrine.However,
disulfiramdoesnotworkforeveryone.Pharmacogeneticstudiesare
revealingvariantsinthegenethatencodestheDBHenzymeand
seemstoinfluencedisulfiram’seffectivenessinreducingcocaine
use. Knowingapatient’sDBHgenotypecouldhelppredictwhether
disulfiramwouldbeaneffectivepharmacotherapyforcocaine
dependenceinthatperson.
Finally,researchershavedevelopedandconductedearlytestsona
cocainevaccinethatcouldhelpreducetheriskofrelapse.Thevaccine
stimulatestheimmunesystemtocreatecocaine-specificantibodies
thatbindtococaine,preventingitfromgettingintothebrain. In
additiontoshowingthevaccine’ssafety,aclinicaltrialfoundthat
patientswhoattainedhighantibodylevelssignificantlyreduced
cocaineuse. However,only38percentofthevaccinatedsubjects
attainedsufficientantibodylevelsandforonly2months.
Researchersareworkingtoimprovethecocainevaccinebyenhancing
thestrengthofbindingtococaineanditsabilitytoelicit
antibodies. Newvaccinetechnologies,includinggenetransferto
boostthespecificityandlevelofantibodiesproducedorenhancethe
metabolismofcocaine,mayalsoimprovetheeffectivenessofthis
treatment. Apharmacogeneticsstudywithasmallnumberof
patientssuggeststhatindividualswithaparticulargenotyperespond
welltothecocainevaccine—anintriguingfindingthatrequiresmore
research.
Inadditiontotreatmentsforaddiction,researchersaredeveloping
medicalinterventionstoaddresstheacuteemergenciesthatresult
fromcocaineoverdose.Oneapproachbeingexploredistheuseof
geneticallyengineeredhumanenzymesinvolvedinthebreakdownof
cocaine,whichwouldcounterthebehavioralandtoxiceffectsofa
cocaineoverdose. Currently,researchersaretestingandrefining
theseenzymesinanimalresearch,withtheultimategoalofmovingto
41–43
41–43
44
45
45
44,46
47
48
49
49

23
clinicaltrials.
BehavioralInterventions
Manybehavioraltreatmentsforcocaineaddictionhaveproventobe
effectiveinbothresidentialandoutpatientsettings.Indeed,behavioral
therapiesareoftentheonlyavailableandeffectivetreatmentsfor
manydrugproblems,includingstimulantaddictions.However,the
integrationofbehavioralandpharmacologicaltreatmentsmay
ultimatelyprovetobethemosteffectiveapproach.
Oneformofbehavioraltherapythatisshowingpositiveresultsin
peoplewithcocaineusedisordersiscontingencymanagement(CM),
alsocalledmotivationalincentives.Programsuseavoucherorprize-
basedsystemthatrewardspatientswhoabstainfromcocaineand
otherdrugs.Onthebasisofdrug-freeurinetests,thepatientsearn
points,orchips,whichcanbeexchangedforitemsthatencourage
healthyliving,suchasagymmembership,movietickets,ordinnerata
localrestaurant.CMmaybeparticularlyusefulforhelpingpatients
achieveinitialabstinencefromcocaineandstayintreatment.
Thisapproachhasrecentlybeenshowntobepracticalandeffectivein
communitytreatmentprograms.
ResearchindicatesthatCMbenefitsdiversepopulationsofcocaine
users.Forexample,studiesshowthatcocaine-dependentpregnant
womenandwomenwithyoungchildrenwhoparticipatedinaCM
programasanadjuncttoothersubstanceusedisordertreatmentwere
abletostayabstinentlongerthanthosewhoreceivedanequivalent
amountofvoucherswithnobehavioralrequirements. Patients
participatinginCMtreatmentforcocaineusewhoalsoexperienced
psychiatricsymptoms—suchasdepression,emotionaldistress,and
hostility—showedasignificantreductionintheseproblems,probably
relatedtoreductionsincocaineuse.
Cognitive-behavioraltherapy(CBT)isaneffectiveapproachfor
preventingrelapse.Thisapproachhelpspatientsdevelopcriticalskills
49
50
39,50–52
51
28
53

24
thatsupportlong-termabstinence—includingtheabilitytorecognize
thesituationsinwhichtheyaremostlikelytousecocaine,avoidthese
situations,andcopemoreeffectivelywitharangeofproblems
associatedwithdruguse.Thistherapycanalsobeusedinconjunction
withothertreatments,therebymaximizingthebenefitsofboth.
Recently,researchersdevelopedacomputerizedformofCBT
(CBT4CBT)thatpatientsuseinaprivateroomofaclinic. This
interactivemultimediaprogramcloselyfollowsthekeylessonsand
skill-developmentactivitiesofin-personCBTinaseriesofmodules.
Moviespresentexamplesandinformationthatsupportthe
developmentofcopingskills;quizzes,games,andhomework
assignmentsreinforcethelessonsandprovideopportunitiestopractice
skills. StudieshaveshownthataddingCBT4CBTtoweekly
counselingboostedabstinence andincreasedtreatmentsuccess
ratesupto6monthsaftertreatment.
Therapeuticcommunities(TCs)—drug-freeresidencesinwhichpeople
inrecoveryfromsubstanceusedisordershelpeachotherto
understandandchangetheirbehaviors—canbeaneffectivetreatment
forpeoplewhousedrugs,includingcocaine. TCsmayrequirea6-to
12-monthstayandcanincludeonsitevocationalrehabilitationand
othersupportiveservicesthatfocusonsuccessfulre-integrationofthe
individualintosociety.TCscanalsoprovidesupportinotherimportant
areas—improvinglegal,employment,andmentalhealthoutcomes.
Regardlessofthespecifictypeofsubstanceusedisordertreatment,it
isimportantthatpatientsreceiveservicesthatmatchalloftheir
treatmentneeds.Forexample,anunemployedpatientwouldbenefit
fromvocationalrehabilitationorcareercounselingalongwithaddiction
treatment.Patientswithmaritalproblemsmayneedcouples
counseling.Onceinpatienttreatmentends,ongoingsupport—also
calledaftercare—canhelppeopleavoidrelapse.Researchindicates
thatpeoplewhoarecommittedtoabstinence,engageinself-help
behaviors,andbelievethattheyhavetheabilitytorefrainfromusing
cocaine(self-efficacy)aremorelikelytoabstain. Aftercareservesto
50
54–56
54–56
54
55
57
57,58
59

25
reinforcethesetraitsandaddressproblemsthatmayincrease
vulnerabilitytorelapse,includingdepressionanddecliningself-
efficacy.
Scientistshavefoundpromisingresultsfromtelephone-based
counselingasalow-costmethodtodeliveraftercare.Forexample,
peoplewhomisusedstimulantswhoparticipatedinsevensessionsof
telephonecounselingshoweddecreasingdruguseduringthefirst3
months,whereasthosewhodidnotreceivecallsincreasedtheiruse.
Voucherincentivescanboostpatients'willingnesstoparticipatein
telephoneaftercare,doublingthenumberofsessionsreceived
accordingtoonestudy.
Community-basedrecoverygroups—suchasCocaineAnonymous—that
usea12-stepprogramcanalsobehelpfulinmaintainingabstinence.
Participantsmaybenefitfromthesupportivefellowshipandfrom
sharingwiththoseexperiencingcommonproblemsandissues.
59
60
61
62

26
Howiscutting-edgescience
helpingusbetterunderstand
addiction?
Twocutting-edgeareasofscience,geneticsandbrainimaging,are
significantlyadvancingourunderstandingofcocaineaddiction.
Researchersestimatethatgeneticscontributes42to79percentofthe
riskforcocaineuseanddependence. Ofcourse,withacomplex
diseasesuchasaddiction,manydifferentgenesareinvolved,andtheir
expressioncanbeinfluencedbytheenvironment.Thereappearstobe
significantoverlapinthegenesthatputpeopleatriskforalladdictive
substances,perhapsindicatingacommonbiologicalpathwayfor
addictionregardlessofthedrug.
Ingenome-wideassociationstudies(GWAS),researchersexamine
whethercertaingenevariantsaremorefrequentlyfoundinpeoplewith
asubstanceusedisorder,whicheventuallymighthelpidentifythoseat
increasedriskfordrugaddiction. Identifyinggeneslinkedto
addictionisonlythefirststep.Candidate-generesearchexaminesthe
linksbetweensubstanceuseandspecificgenesthatencodeproteins
thatappeartoberelatedtoaddiction.Forexample,researchershave
foundconnectionsbetweenvariousaspectsofcocaineaddictionand
thegenesthatencodeforparticulardopaminereceptorsandthe
enzymesthatbreakdownthisneurotransmitter.
Becauseenvironmentalfactorstypicallyshapetheimpactofgeneson
diseaserisk,researchersmustalsoidentifyhowparticulargene-by-
environmentinteractionsinfluencethecourseofaddiction. Research
inthefieldofepigeneticsisuncoveringhowtheenvironmentinduces
long-termchangesingeneexpression—influencingthepatternofgene
expression—withoutalteringtheDNAsequence.
63
63
64,65
63
63
66

27
Inanimalresearch,scientistsaredetermininghowlong-termcocaine
exposurechangesgeneexpressioninthebrain,particularlyinthe
rewardpathway.Studieshavelinkedspecificcocaine-induced
epigeneticchangestoneuroadaptations andbehavioralhallmarksof
addiction,suchassensitivitytococaine’srewardingeffects. The
epigeneticchangesinducedbycocainecanbepassedtothenext
generation,evenifthedrugexposuredoesnotoccurprenatally.
Althoughmuchmoregeneticandepigeneticresearchisneeded,
understandingaddictionatthemolecularleveloffersgreatpromisefor
improvingdiagnosis,forexamplebydiscoveringbiomarkersfor
diseaseseverityortreatmentresponse.
Althoughmoreresearchisneeded,brain-imagingmightbeusedto
detectbiomarkersfordrugaddictionvulnerability,asthese
technologieshaveyieldedinsightsintotheprocessesunderlying
cravingandhowmedicationsmayquellthebrain’sresponsetococaine
cues. Arelativelynewneuroimagingtechnologycalleddefault-mode
orresting-statefunctionalmagneticresonanceimaging(rs-fMRI)
revealsbrainactivitywhenpeoplearealertbutnotperforminga
particulartask;researchersusethistechniquetocomparefunctional
brainnetworksofpeoplewhohaveusedcocaineforalongtimeand
thosewhohavenot.Thesestudiessuggestthatthereisreduced
connectivitybetweenvariousbraincircuits andbetweenthetwo
hemispheres amongpeoplewithcocainedependence.Researchers
havealsocorrelatedreducedconnectivitybetweenparticularbrain
circuitswithimportantaddiction-relatedbehaviors,includingriskfor
relapse andimpulsivity.
Neuroimagingtechnologiesarealsodocumentinghowthebrainsof
cocaineusersmayrecoverafterperiodsofabstinence.Forexample,
thesetechniquesindicatethatyearsofcocaineuseareassociatedwith
reducedgreymatterinparticularbrainregions.However,peoplewho
maintainedcocaineabstinenceforapproximately9monthsshowed
greymatterlevelssimilartoorgreaterthanthoseofpeoplewhohad
neverusedthedrug. Furtheranalysisindicatedthattheincreased
greymatteroccurredinregionsotherthantheonesalteredbycocaine
use,suggestingthattheneurobiologicalchangesinvolvedinrecovery
67
66,67
68
66
69
70–72
73
71 72
74

28
aremorecomplexthansimplyreversingthechangesrelatedto
addiction. Theresearchersalsofoundthatincreasedgreymatter
volumeinbrainregionsinvolvedwithbehavioralcontrolwere
associatedwithlongerdurationofabstinence.
fMRItechnologieshavealsorevealedthatabstinencefromcocainehas
important,restorativeeffectsonthebrain.Althoughcurrentcocaine
usersdemonstratedreducedbrainactivityinabraincircuitthat
mediatesresponseinhibitionduringamotorcontroltask,individuals
whohadattainedabstinenceforanaverageof8monthsshowed
similarpatternsofactivationandlevelsofperformancetothosewho
hadneverusedthedrug. Theresultssuggestthatabstinencehelps
restorethefunctioningofthisbraincircuit.
Researchersareengagedinseverallarge-scale,collaborativeprojects
tomapthehumanconnectome,whichisthebrain’snetworkof
interconnectedcircuits.Forexample,theNationalInstitutesofHealth
supportstheHumanConnectomeProjecttogeneratemapsofthe
developing,adult,andagingbrain.Byhavingamapofthetypical
brain,scientistswillfurtherunderstandhowneuralfunctioningdiffers
inbehavioraldisorders—knowledgethatwilldriveimproved
diagnosticsandtreatments.
74
74
75

29
References
1. CalatayudJ,GonzálezA.Historyofthedevelopmentandevolution
oflocalanesthesiasincethecocaleaf.Anesthesiology.
2003;98(6):1503-1508.
2. GoldsteinRA,DesLauriersC,BurdaAM.Cocaine:history,social
implications,andtoxicity–areview.Dis–MonDM.2009;55(1):6-38.
doi:10.1016/j.disamonth.2008.10.002.
3. DrentM,WijnenP,BastA.Interstitiallungdamageduetococaine
abuse:pathogenesis,pharmacogenomicsandtherapy.CurrMed
Chem.2012;19(33):5607-5611.
4. CenterforBehavioralHealthStatisticsandQuality(CBHSQ).
BehavioralHealthTrendsintheUnitedStates:Resultsfromthe
2014NationalSurveyonDrugUseandHealth.Rockville,MD:
SubstanceAbuseandMentalHealthServicesAdministration;
2015.HHSPublicationNo.SMA15-4927,NSDUHSeriesH-50.
5. JohnstonL,O’MalleyP,MiechR,BachmanJ,SchulenbergJ.
MonitoringtheFutureNationalSurveyResultsonDrugUse:1975-
2015:Overview:KeyFindingsonAdolescentDrugUse.AnnArbor,
MI:InstituteforSocialResearch,TheUniversityofMichigan;2015.
6. CenterforBehavioralHealthStatisticsandQuality(CBHSQ).Drug
AbuseWarningNetwork:2011:SelectedTablesofNational
EstimatesofDrug-RelatedEmergencyDepartmentVisits.
Rockville,MD:SubstanceAbuseandMentalHealthServices
Administration;2013.
7. RiezzoI,FioreC,DeCarloD,etal.Sideeffectsofcocaineabuse:
multiorgantoxicityandpathologicalconsequences.CurrMed
Chem.2012;19(33):5624-5646.
8. BaikJ-H.Dopaminesignalinginreward-relatedbehaviors.Front
NeuralCircuits.2013;7.doi:10.3389/fncir.2013.00152.
9. SchmidtHD,PierceRC.Cocaine-inducedneuroadaptationsin
glutamatetransmission:potentialtherapeutictargetsforcraving

30
andaddiction.AnnNYAcadSci.2010;1187:35-75.
doi:10.1111/j.1749-6632.2009.05144.x.
10. WolfME.TheBermudaTriangleofcocaine-induced
neuroadaptations.TrendsNeurosci.2010;33(9):391-398.
doi:10.1016/j.tins.2010.06.003.
11. MantschJR,VranjkovicO,TwiningRC,GasserPJ,McReynoldsJR,
BlacktopJM.Neurobiologicalmechanismsthatcontributetostress-
relatedcocaineuse.Neuropharmacology.2014;76,PartB:383-
394.doi:10.1016/j.neuropharm.2013.07.021.
12. LucantonioF,StalnakerTA,ShahamY,NivY,SchoenbaumG.The
impactoforbitofrontaldysfunctiononcocaineaddiction.Nat
Neurosci.2012;15(3):358-366.doi:10.1038/nn.3014.
13. LucantonioF,TakahashiYK,HoffmanAF,etal.Orbitofrontal
activationrestoresinsightlostaftercocaineuse.NatNeurosci.
2014;17(8):1092-1099.doi:10.1038/nn.3763.
14. SpronkDB,vanWelJHP,RamaekersJG,VerkesRJ.Characterizing
thecognitiveeffectsofcocaine:acomprehensivereview.Neurosci
BiobehavRev.2013;37(8):1838-1859.
doi:10.1016/j.neubiorev.2013.07.003.
15. AdvokatC,ComatyJ,JulienR.Julien’sPrimerofDrugAction.13th
ed.NewYork,NY:WorthPublishers;2014.
16. FonsecaAC,FerroJM.Drugabuseandstroke.CurrNeurolNeurosci
Rep.2013;13(2):325.doi:10.1007/s11910-012-0325-0.
17. PenningsEJM,LecceseAP,WolffFAde.Effectsofconcurrentuseof
alcoholandcocaine.AddictAbingdonEngl.2002;97(7):773-783.
18. BüttnerA.Neuropathologicalalterationsincocaineabuse.Curr
MedChem.2012;19(33):5597-5600.
19. Mateos-GarcíaA,Roger-SánchezC,Rodriguez-AriasM,etal.
Highersensitivitytotheconditionedrewardingeffectsofcocaine
andMDMAinHigh-Novelty-Seekersmiceexposedtoacocaine
bingeduringadolescence.Psychopharmacology(Berl).
2015;232(1):101-113.doi:10.1007/s00213-014-3642-y.

31
20. MarajS,FigueredoVM,LynnMorrisD.Cocaineandtheheart.Clin
Cardiol.2010;33(5):264-269.doi:10.1002/clc.20746.
21. SinhaR.Theclinicalneurobiologyofdrugcraving.CurrOpin
Neurobiol.2013;23(4):649-654.doi:10.1016/j.conb.2013.05.001.
22. KhalsaJH,ElkashefA.InterventionsforHIVandhepatitisCvirus
infectionsinrecreationaldrugusers.ClinInfectDis.
2010;50(11):1505-1511.doi:10.1086/652447.
23. BuchS,YaoH,GuoM,etal.CocaineandHIV-1interplayinCNS:
cellularandmolecularmechanisms.CurrHIVRes.2012;10(5):425-
428.
24. ParikhN,NonnemacherMR,PirroneV,BlockT,MehtaA,Wigdahl
B.Substanceabuse,HIV-1andhepatitis.CurrHIVRes.
2012;10(7):557-571.
25. WendellAD.Overviewandepidemiologyofsubstanceabusein
pregnancy.ClinObstetGynecol.2013;56(1):91-96.
doi:10.1097/GRF.0b013e31827feeb9.
26. CainMA,BornickP,WhitemanV.Thematernal,fetal,andneonatal
effectsofcocaineexposureinpregnancy.ClinObstetGynecol.
2013;56(1):124-132.doi:10.1097/GRF.0b013e31827ae167.
27. HullL,MayJ,Farrell-MooreD,SvikisDS.Treatmentofcocaine
abuseduringpregnancy:translatingresearchtoclinicalpractice.
CurrPsychiatryRep.2010;12(5):454-461.doi:10.1007/s11920-
010-0138-2.
28. SchottenfeldRS,MooreB,PantalonMV.Contingencymanagement
withcommunityreinforcementapproachortwelve-stepfacilitation
drugcounselingforcocainedependentpregnantwomenor
womenwithyoungchildren.DrugAlcoholDepend.
2011;118(1):48-55.doi:10.1016/j.drugalcdep.2011.02.019.
29. BehnkeM,SmithVC,AbuseConS,NewbornConFA.Prenatal
substanceabuse:short-andlong-termeffectsontheexposed
fetus.Pediatrics.2013;131(3):e1009-e1024.
doi:10.1542/peds.2012-3931.

32
30. GouinK,MurphyK,ShahPS,KnowledgeSynthesisgroupon
DeterminantsofLowBirthWeightandPretermBirths.Effectsof
cocaineuseduringpregnancyonlowbirthweightandpreterm
birth:systematicreviewandmetaanalyses.AmJObstetGynecol.
2011;204(4):340.e1-e12.doi:10.1016/j.ajog.2010.11.013.
31. LambertBL,BauerCR.Developmentalandbehavioral
consequencesofprenatalcocaineexposure:areview.JPerinatol
OffJCalifPerinatAssoc.2012;32(11):819-828.
doi:10.1038/jp.2012.90.
32. LesterBM,LagasseLL.Childrenofaddictedwomen.JAddictDis.
2010;29(2):259-276.doi:10.1080/10550881003684921.
33. AckermanJP,RigginsT,BlackMM.Areviewoftheeffectsof
prenatalcocaineexposureamongschool-agedchildren.Pediatrics.
2010;125(3):554-565.doi:10.1542/peds.2009-0637.
34. Buckingham-HowesS,BergerSS,ScalettiLA,BlackMM.
Systematicreviewofprenatalcocaineexposureandadolescent
development.Pediatrics.2013;131(6):e1917-e1936.
doi:10.1542/peds.2012-0945.
35. LiK,ZhuD,GuoL,etal.Connectomicssignaturesofprenatal
cocaineexposureaffectedadolescentbrains.HumBrainMapp.
2013;34(10):2494-2510.doi:10.1002/hbm.22082.
36. CenterforBehavioralHealthStatisticsandQuality(CBHSQ).
TreatmentEpisodeDataSet(TEDS):2003-2013.National
AdmissionstoSubstanceAbuseTreatmentServices.Rockville,
MD:SubstanceAbuseandMentalHealthServicesAdministration;
2015.BHSISSeriesS-75,HHSPublicationNo.(SMA)15-4934.
37. ShorterD,DomingoCB,KostenTR.Emergingdrugsforthe
treatmentofcocaineusedisorder:areviewofneurobiological
targetsandpharmacotherapy.ExpertOpinEmergDrugs.
2015;20(1):15-29.doi:10.1517/14728214.2015.985203.
38. KarilaL,ReynaudM,AubinH-J,etal.Pharmacologicaltreatments
forcocainedependence:istheresomethingnew?CurrPharmDes.
2011;17(14):1359-1368.

33
39. KampmanKM.What’snewinthetreatmentofcocaineaddiction?
CurrPsychiatryRep.2010;12(5):441-447.doi:10.1007/s11920-
010-0143-5.
40. Harvey-LewisC,LiZ,HigginsGA,FletcherPJ.The5-HT2Creceptor
agonistlorcaserinreducescocaineself-administration,
reinstatementofcocaine-seekingandcocaineinducedlocomotor
activity.Neuropharmacology.2016;101:237-245.
doi:10.1016/j.neuropharm.2015.09.028.
41. ShorterD,NielsenDA,HuangW,HardingMJ,HamonSC,Kosten
TR.Pharmacogeneticrandomizedtrialforcocaineabuse:
disulfiramandα1A-adrenoceptorgenevariation.Eur
NeuropsychopharmacolJEurCollNeuropsychopharmacol.
2013;23(11):1401-1407.doi:10.1016/j.euroneuro.2013.05.014.
42. SpellicyCJ,KostenTR,HamonSC,HardingMJ,NielsenDA.ANKK1
andDRD2pharmacogeneticsofdisulfiramtreatmentforcocaine
abuse.PharmacogenetGenomics.2013;23(7):333-340.
doi:10.1097/FPC.0b013e328361c39d.
43. KostenTR,WuG,HuangW,etal.Pharmacogeneticrandomized
trialforcocaineabuse:disulfiramanddopamineβ-hydroxylase.
BiolPsychiatry.2013;73(3):219-224.
doi:10.1016/j.biopsych.2012.07.011.
44. KostenTR,DomingoCB.Canyouvaccinateagainstsubstance
abuse?ExpertOpinBiolTher.2013;13(8):1093-1097.
doi:10.1517/14712598.2013.791278.
45. MartellBA,OrsonFM,PolingJ,etal.Cocainevaccineforthe
treatmentofcocainedependenceinmethadone-maintained
patients:arandomized,double-blind,placebo-controlledefficacy
trial.ArchGenPsychiatry.2009;66(10):1116-1123.
doi:10.1001/archgenpsychiatry.2009.128.
46. CaiX,TsuchikamaK,JandaKD.Modulatingcocainevaccine
potencythroughhaptenfluorination.JAmChemSoc.
2013;135(8):2971-2974.doi:10.1021/ja400356g.
47. BrimijoinS,ShenX,OrsonF,KostenT.Prospects,promiseand
problemsontheroadtoeffectivevaccinesandrelatedtherapies

34
forsubstanceabuse.ExpertRevVaccines.2013;12(3):323-332.
doi:10.1586/erv.13.1.
48. NielsenDA,HamonSC,KostenTR.Theκ-opioidreceptorgeneasa
predictorofresponseinacocainevaccineclinicaltrial.Psychiatr
Genet.2013;23(6):225-232.doi:10.1097/YPG.0000000000000008.
49. SchindlerCW,GoldbergSR.Acceleratingcocainemetabolismas
anapproachtothetreatmentofcocaineabuseandtoxicity.Future
MedChem.2012;4(2):163-175.doi:10.4155/fmc.11.181.
50. PenberthyJK,Ait-DaoudN,VaughanM,FanningT.Reviewof
treatmentforcocainedependence.CurrDrugAbuseRev.
2010;3(1):49-62.
51. PetryNM,BarryD,AlessiSM,RounsavilleBJ,CarrollKM.A
randomizedtrialadaptingcontingencymanagementtargets
basedoninitialabstinencestatusofcocaine-dependentpatients.J
ConsultClinPsychol.2012;80(2):276-285.doi:10.1037/a0026883.
52. SchierenbergA,vanAmsterdamJ,vandenBrinkW,GoudriaanAE.
Efficacyofcontingencymanagementforcocainedependence
treatment:areviewoftheevidence.CurrDrugAbuseRev.
2012;5(4):320-331.
53. PetryNM,AlessiSM,RashCJ.Contingencymanagement
treatmentsdecreasepsychiatricsymptoms.JConsultClinPsychol.
2013;81(5):926-931.doi:10.1037/a0032499.
54. CarrollKM,BallSA,MartinoS,etal.Computer-assisteddeliveryof
cognitive-behavioraltherapyforaddiction:arandomizedtrialof
CBT4CBT.AmJPsychiatry.2008;165(7):881-888.
doi:10.1176/appi.ajp.2008.07111835.
55. CarrollKM,BallSA,MartinoS,NichC,BabuscioTA,RounsavilleBJ.
Enduringeffectsofacomputer-assistedtrainingprogramfor
cognitivebehavioraltherapy:a6-monthfollow-upofCBT4CBT.
DrugAlcoholDepend.2009;100(1-2):178-181.
doi:10.1016/j.drugalcdep.2008.09.015.
56. CarrollKM,KilukBD,NichC,etal.Computer-assisteddeliveryof
cognitive-behavioraltherapy:efficacyanddurabilityofCBT4CBT

35
amongcocaine-dependentindividualsmaintainedonmethadone.
AmJPsychiatry.2014;171(4):436-444.
doi:10.1176/appi.ajp.2013.13070987.
57. VanderplasschenW,ColpaertK,AutriqueM,etal.Therapeutic
communitiesforaddictions:areviewoftheireffectivenessfroma
recovery-orientedperspective.SciWorldJ.2013;2013,
2013:e427817.doi:10.1155/2013/427817.
58. LeonGD.Isthetherapeuticcommunityanevidencebased
treatment?Whattheevidencesays.TherCommunitiesInt
JdournalTherSupportOrgan.2010;31(2):104-128.
59. McKayJR,VanHornD,RennertL,DrapkinM,IveyM,Koppenhaver
J.Factorsinsustainedrecoveryfromcocainedependence.JSubst
AbuseTreat.2013;45(2):163-172.doi:10.1016/j.jsat.2013.02.007.
60. FarabeeD,CousinsSJ,BrechtM-L,etal.Acomparisonoffour
telephone-basedcounselingstylesforrecoveringstimulantusers.
PsycholAddictBehav.2013;27(1):223-229.
doi:10.1037/a0029572.
61. VanHornDHA,DrapkinM,IveyM,etal.Voucherincentives
increasetreatmentparticipationintelephone-basedcontinuing
careforcocainedependence.DrugAlcoholDepend.2011;114(2-
3):225-228.doi:10.1016/j.drugalcdep.2010.09.007.
62. DonovanDM,DaleyDC,BrighamGS,etal.Stimulantabuser
groupstoengagein12-step:amultisitetrialintheNational
InstituteonDrugAbuseClinicalTrialsNetwork.JSubstAbuse
Treat.2013;44(1):103-114.doi:10.1016/j.jsat.2012.04.004.
63. AgrawalA,VerweijKJH,GillespieNA,etal.Thegeneticsof
addiction-atranslationalperspective.TranslPsychiatry.
2012;2:e140.doi:10.1038/tp.2012.54.
64. DrgonT,ZhangP-W,JohnsonC,etal.Genomewideassociation
foraddiction:replicatedresultsandcomparisonsoftwoanalytic
approaches.PloSOne.2010;5(1):e8832.
doi:10.1371/journal.pone.0008832.
65. KreekMJ,LevranO,ReedB,SchlussmanSD,ZhouY,ButelmanER.

36
Opiateaddictionandcocaineaddiction:underlyingmolecular
neurobiologyandgenetics.JClinInvest.2012;122(10):3387-3393.
doi:10.1172/JCI60390.
66. NestlerEJ.Epigeneticmechanismsofdrugaddiction.
Neuropharmacology.2014;76PtB:259-268.
doi:10.1016/j.neuropharm.2013.04.004.
67. SchmidtHD,McGintyJF,WestAE,Sadri-VakiliG.Epigeneticsand
psychostimulantaddiction.ColdSpringHarbPerspectMed.
2013;3(3):a012047.doi:10.1101/cshperspect.a012047.
68. VassolerFM,Sadri-VakiliG.Mechanismsoftransgenerational
inheritanceofaddictive-likebehaviors.Neuroscience.
2014;264:198-206.doi:10.1016/j.neuroscience.2013.07.064.
69. YoungKA,FranklinTR,RobertsDCS,etal.Nippingcuereactivityin
thebud:baclofenpreventslimbicactivationelicitedbysubliminal
drugcues.JNeurosciOffJSocNeurosci.2014;34(14):5038-5043.
doi:10.1523/JNEUROSCI.4977-13.2014.
70. GuH,SalmeronBJ,RossTJ,etal.Mesocorticolimbiccircuitsare
impairedinchroniccocaineusersasdemonstratedbyresting-
statefunctionalconnectivity.NeuroImage.2010;53(2):593-601.
doi:10.1016/j.neuroimage.2010.06.066.
71. McHughMJ,DemersCH,SalmeronBJ,DevousMD,SteinEA,
AdinoffB.Cortico-amygdalacouplingasamarkerofearlyrelapse
riskincocaine-addictedindividuals.FrontPsychiatry.2014;5:16.
doi:10.3389/fpsyt.2014.00016.
72. WisnerKM,PatzeltEH,LimKO,MacDonaldAW.Anintrinsic
connectivitynetworkapproachtoinsula-deriveddysfunctions
amongcocaineusers.AmJDrugAlcoholAbuse.2013;39(6):403-
413.doi:10.3109/00952990.2013.848211.
73. KellyC,ZuoX-N,GotimerK,etal.Reducedinterhemispheric
restingstatefunctionalconnectivityincocaineaddiction.Biol
Psychiatry.2011;69(7):684-692.
doi:10.1016/j.biopsych.2010.11.022.
74. ConnollyCG,BellRP,FoxeJJ,GaravanH.Dissociatedgreymatter

37
changeswithprolongedaddictionandextendedabstinencein
cocaineusers.PLoSONE.2013;8(3):e59645.
doi:10.1371/journal.pone.0059645.
75. BellRP,FoxeJJ,RossLA,GaravanH.Intactinhibitorycontrol
processesinabstinentdrugabusers(I):afunctionalneuroimaging
studyinformercocaineaddicts.Neuropharmacology.
2014;82:143-150.doi:10.1016/j.neuropharm.2013.02.018.

38
WherecanIgetfurther
informationaboutcocaine?
Tolearnmoreaboutcocaineandotherdrugsofabuse,visittheNIDA
websiteatwww.drugabuse.govorcontactDrugPubsat877-NIDA-NIH
(877-643-2644;TTY/TDD:240-645-0228).
NIDA'swebsiteincludes:
Informationondrugsofabuseandrelatedhealthconsequences
NIDApublications,news,andevents
Resourcesforhealthcareprofessionals,educators,andpatients
andfamilies
InformationonNIDAresearchstudiesandclinicaltrials
Fundinginformation(includingprogramannouncementsand
deadlines)
Internationalactivities
Linkstorelatedwebsites(accesstowebsitesofmanyother
organizationsinthefield)
InformationinSpanish(enespañol)
NIDAwebsitesandwebpages
www.drugabuse.gov
www.teens.drugabuse.gov
www.easyread.drugabuse.gov
www.drugabuse.gov/drugs-abuse/cocaine
www.researchstudies.drugabuse.gov

39
www.irp.drugabuse.gov
Forphysicianinformation
NIDAMED:www.drugabuse.gov/nidamed
Otherwebsites
Informationoncocaineabuseisalsoavailablethroughthefollowing
Website:
SubstanceAbuseandMentalHealthServices
Administration:www.samhsa.gov
DrugEnforcementAdministration:www.dea.gov
MonitoringtheFuture:www.monitoringthefuture.org/
ThePartnershipatDrugFree.org:www.drugfree.org/drug-guide
Thispublicationisavailableforyouruseandmaybereproducedin
itsentiretywithoutpermissionfromNIDA.Citationofthesource
isappreciated,usingthefollowinglanguage:Source:National
InstituteonDrugAbuse;NationalInstitutesofHealth;U.S.
DepartmentofHealthandHumanServices.

{kind=link}
{kind=link}
{kind=link}
{kind=link}