
Estimating the Failure Risk of Quarantine Systems for Preventing COVID-
19 Outbreaks in Australia and New Zealand
Leah Grout,
1*
Ameera Katar,
2
Driss Ait Ouakrim,
2
Jennifer A. Summers,
1
Amanda
Kvalsvig,
1
Michael G. Baker,
1
Tony Blakely,
2
Nick Wilson
1
1
Department of Public Health, University of Otago Wellington, New Zealand
2
Melbourne School of Population and Global Health, University of Melbourne, Melbourne,
Australia
* Corresponding author: leah.grout@otago.ac.nz
Abstract
Objectives: To identify COVID-19 outbreaks and border control failures associated with
quarantine systems in Australia and New Zealand and to estimate the failure risks.
Design, setting, participants: Observational epidemiological study of travellers transiting
quarantine in Australia and New Zealand up to 31 March 2021.
Main outcome measures: The incidence of COVID-19 related failures arising from
quarantine, and the failure risk for those transiting quarantine, estimated both per 100,000
travellers and per 1000 SARS-CoV-2 positive cases.
Results: Australia and New Zealand had 24 COVID-19 related failures arising from
quarantine systems up to 31 March 2021 (14 and 10, respectively). One resultant outbreak
involved an estimated 800 deaths and quarantine failures instigated nine lockdowns. The
failure risk for those transiting quarantine was estimated at 6.3 failures per 100,000 travellers
and 5.8 failures (95%CI: 3.5 to 8.1) per 1000 SARS-CoV-2 positive cases. The latter risk was
three-fold higher in New Zealand compared with Australia. Approximately 55% of
quarantine system failures could likely have been prevented with the full vaccination of
frontline border workers, for 70% effectiveness at preventing transmission.
Conclusions: Quarantine system failures can be costly in terms of lives and economic
impacts such as lockdowns. Ongoing improvements or alternatives to hotel-based quarantine
are required.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint
NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice.
Introduction
New Zealand and Australian states have successfully eliminated community transmission of
the pandemic virus SARS-CoV-2,
1
albeit with occasional outbreaks from imported cases that
have typically been quickly brought under control. These two countries have primarily used
hotel-based quarantine for citizens returning to their countries during the pandemic period,
with 14 days of quarantine combined with PCR testing and mask use in any shared spaces
(eg, common exercise areas used in New Zealand, but not in most Australian states).
Converting hotels for quarantine purposes has the advantage of making use of a resource that
would otherwise be underused during a pandemic, given declines in international tourism.
However, the major disadvantage of hotel-based quarantine is that it is likely to be less
effective than purpose-built quarantine facilities owing to shared spaces and lack of safe
ventilation (as per WHO advice on air flow
2
). Moreover, the consequences of leakage of the
virus out of quarantine (eg, through facility workers) may be more severe given higher
population density in urban settings where the hotels are located. Given these issues, we
aimed to estimate the failure risk of quarantine systems in New Zealand and Australia in
terms of the spread of COVID-19 infection into the community.
As of 31 March 2021, the rolling 7-day average number of COVID-19 vaccine doses
administrated per 100 people was 0.18 in Australia and 0.08 in New Zealand
3
However, this
was counted as single vaccine doses and does not equal the total number of people vaccinated
(eg, the Pfizer/BioNTech vaccine which is currently used in New Zealand requires two
doses).
3
The majority of border workers in Australia and New Zealand have been vaccinated
(eg, over 56,000 doses had been administered to border workers as of 28 March,
4
and all
hotel quarantine workers in Victoria who have face-to-face contact with returned travellers
received their first dose of the vaccine by the first week in April
5
).
Methods
We defined a quarantine system failure as where a border/health worker or person in the
community with a link to the quarantine/isolation system, became infected with SARS-CoV-
2. This definition included people infected in hospital from cases who had been transferred
from a quarantine facility (as such cases were still in the 14-day quarantine process). But this
definition did not include pandemic virus transmission between returnees within the
quarantine facilities (as some other commentators have included in lists of failures in the
Australian context
6
).
We searched official websites in both countries, and for the eight states and territories in
Australia, to identify outbreaks and border control failures associated with quarantine systems
(searches conducted between 6 January and 29 April 2021). Where an outbreak source was
uncertain (eg, the Auckland, New Zealand, August 2020 outbreak) we used the best available
evidence to classify it as a quarantine failure or not. We used two denominators: a) the
estimated number of travellers who went through quarantine facilities during the 2020 year
up to 31 March 2021; and b) the number of SARS-CoV-2 positive people who went through
these facilities in this same time period. The unit of analyses were New Zealand, the eight
Australian states and territories, and both countries combined.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint
For New Zealand, we used official data on both travellers going through the quarantine
system,
7
along with official (Ministry of Health) data on SARS-CoV-2 positive cases,
8
although there are some discrepancies in the information about when regular testing began in
Managed Isolation and Quarantine (MIQ) facilities. For Australia we used overseas arrival
data
9
and health data.
10 11
Results
The collated data for quarantine system failures is shown in Table 1, with specific details of
each event in the Appendix (Table A1). In Australia, 14 failures were identified, one causing
over 800 deaths (Victoria’s second wave) and eight out of the 14 resulting in lockdowns. In
New Zealand, there were ten failures, with one causing an outbreak with three deaths, and
also a lockdown.
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

Table 1: Identified quarantine system failures in Australia and New Zealand during the COVID-19 pandemic, the relevant denominator populations
and estimated failure risks (with numerator and denominator data up to 31 March 2021)
Jurisdiction
Identified
quarantine
system failures
Travellers
experiencing
quarantine/
isolation
Active cases
of SARS-
CoV-2
infection
identified in
quarantine
Failure risk
per 100,000
travellers
going
through
quarantine
Failure risk
per 1000
positive cases
in
quarantine*
(95%CI) Comments
New Zealand 10 127,730 758 7.8 13.2
(5.0 to 21.4)
From 17 June 2020 (date of the first positive test in a
quarantine facility) until 31 March 2021, excluding 9 cases
with no history of overseas travel.
8
Australian States and Territories
Australian Capital
Territory (ACT)
0 765 25 0.0 0.0
Queensland 3 40,896 543 7.3 5.5 Two of the failures occurred at a hospital during the
quarantine process.
New South Wales 5 128,646 1,581 3.9 3.2
Northern Territory 0 9,180 88 0.0 0.0 Includes a non-hotel facility (a former workers’ camp)
12
South Australia 1 13,023 230 7.7 4.3
Tasmania 0 405 21 0.0 0.0
Victoria 4 33,300 462 12.0 8.7 Victoria suspended flights from 14 February to 25 March
2021 due to the Holiday Inn cluster, where an illegal
nebuliser allegedly caused a quarantine failure and resulted
in 14 cases.
Western Australia 1 29,383 450 3.4 2.2
All of Australia 14 255,598 3,400 5.5 4.1
(2.0 to 6.3)
These only included cases diagnosed between 1 April 2020
until 31 March 2021.
Relative risk (New Zealand : Australia)
3.2 (1.4 to
7.2)
P-value = 0.0081 (Mid-P exact, 2-tailed test)
New Zealand and Australia
Both countries
combined
24 383,328 4,158 6.3 5.8
(3.5 to 8.1)
* 95% confidence intervals are shown in parentheses for country-level risks only; state-level risks with zeros or low numbers are too sparse
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint
Given our estimates of the number of travellers processed via quarantine systems (Table 1),
the overall risks for both countries combined were one failure per 15,972 travellers, and one
failure per 173 SARS-CoV-2 positive cases in quarantine. The combined data can also be
interpreted as one outbreak leading to a lockdown response per 42,592 travellers; and
approximately one death from COVID-19 per 477 travellers (using the 800 deaths estimate
from Australia and the three deaths from New Zealand – although this figure is largely driven
by the second wave in Victoria and is unlikely generalizable forward in time).
At the country level, there were 13.2 failures per 1000 SARS-CoV-2 positive cases transiting
quarantine in New Zealand (95% confidence interval [CI]: 5.0 to 21.4), compared to 4.1 per
1000 SARS-CoV-2 positive cases in Australia (95%CI: 2.0 to 6.3) – a three-fold difference in
risk (relative risk: 3.2, 95%CI: 1.4 to 7.2). Approximately 55.4% of quarantine system
failures could have been preventable with the full vaccination of frontline border workers
(Table A1) due to the combined effects of vaccination lowering the risk of getting infected by
70% or more (as in the case of the Moderna vaccine
13
), and the lesser duration of infectivity
and lower peak infectivity for those infected.
14
Discussion
This analysis identified 24 failures of quarantine systems in Australia and New Zealand
combined (up to 31 March 2021). The significantly higher failure risk per 1000 SARS-CoV-2
positive cases transiting quarantine in New Zealand versus Australia could reflect a lower
quality approach in the former, with perhaps some of the difference due to greater detection
in New Zealand from more border worker testing over a longer period.
These estimates are subject to chance variations due to the low numbers of failures. These
estimates will also probably be an underestimate of all quarantine breaches, as not all of those
infected will transmit the virus and start a detectable chain of transmission. Genomes of the
first 649 viral isolates collected in New Zealand show that only 19% of virus introductions
resulted in ongoing transmission of more than one additional case.
15
Therefore, counts of
border failures are sensitive to how they are identified and defined. Indeed, with increased
testing (eg, testing of people after leaving quarantine on day 16 as is now common in
Australia), we may be detecting breaches that previously would have been undetected.
Looking forward, the failure risks per month in New Zealand and Australia may increase,
given that the proportion of travellers returning to these countries who are infected is
increasing due to global intensification of the pandemic and the increasing infectivity of new
SARS-CoV-2 variants.
16
Indeed, there have been several clearly documented cases of spread
within quarantine hotels (eg, two instances in Melbourne in February 2021, two instances in
Sydney in April 2021), highlighting the increased risk and evolving situation with more
highly infectious variants arriving from overseas.
However, offsetting this trend will be measures such as the vaccination of quarantine
workers. In New Zealand, the vaccination of border workers began in February 2021 with the
Pfizer/BioNTech vaccine. However, vaccination does not fully protect against SARS-CoV-2
transmission, although a moderate degree of protection is likely. For example, infection rates
were halved for the AstraZeneca vaccine,
17 18
and perhaps reduced by 70% for the Moderna
mRNA vaccine, as indicated by using swab results for asymptomatic infection plus
symptomatic cases.
13
For vaccinated people who are infected, primate study evidence
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint
suggests (consistent with expectation) that the infectivity is decreased in peak and duration,
14
further protecting the border.
Furthermore, the level of testing of quarantine workers has been increasing (eg,
19
; which will
find some failures before they have a chance to establish as an outbreak in the community).
There have been other improvements in the quarantine systems over time (eg, improved
security, introduction of mask wearing within quarantine settings, reduction in shared spaces,
improved PPE used by workers, and other procedures as detailed in both countries
20 21
).
Another risk reduction practice would be using better or purpose-built facilities in rural
locations as these have less risk from close contacts in central business district hotels and
within-building spread from poor ventilation systems. Limitations of our analysis include
residual uncertainty around the cause of some outbreaks (eg, the Auckland August 2020), and
imprecision with denominator data on traveller numbers for Australia (eg, some travellers
were moved between states on domestic flights which is not captured in the official data we
used). Additionally, case numbers are constantly changing, due to the number of
reclassifications caused by false positives and duplications.
To substantially reduce the risk of SARS-CoV-2 incursion out of quarantine (until such time
as enough of the population is vaccinated), the most obvious action is to reduce arrivals, or
even suspend arrivals, from high infection locations (as New Zealand temporarily did for
travel from India and other high risk countries in April 2021
22
). Beyond this, there are a range
of other potential improvements in ongoing arrangements and processes as detailed in Table
2. Furthermore, the start of quarantine-free travel between Australia and New Zealand (also
known as a "green zone") in April 2021 provides an opportunity to benchmark COVID-19
border control policies and practices, identify potential improvements in both countries, and
harmonise best practices across the region. The green zone further intertwines the biosecurity
status of both nations and it is therefore even more important to lower the risk of border
failures that could disrupt such travel. This shift from a one-size-fits-all strategy to a risk-
based approach to border management can be summarised as a 'traffic light' approach.
23
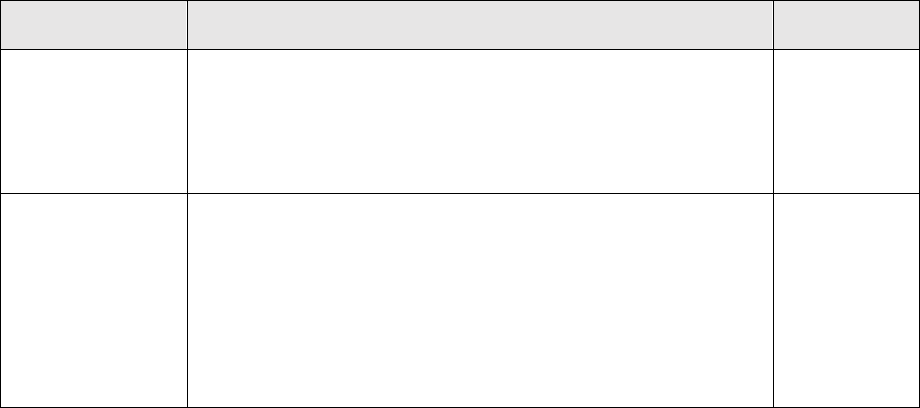
Table 2: List of potential policy and operational options for improved COVID-19 control
associated with quarantine systems in Australia and New Zealand, including measures to
reduce the numbers of infected people arriving into quarantine facilities
Policy option Description
Our priority
rankings
1. Cap travel from
high prevalence
countries and/or
suspend for a
period
Reduce the in-flow of travellers by reducing or suspending flights
to Australia and New Zealand (NZ) from very high incidence
countries where the pandemic is out of control. These governments
have the legal powers to put conditions on the existing rights of
their citizens to enter their country of citizenship (ie, on public
health grounds).
Top priority
2. Pre-departure
testing plus/minus
pre-departure
quarantine
Expand existing requirements for pre-departure testing to additional
traveller source countries. Pre-departure testing could be expanded
from not only a PCR test within 72 hours of departure to also add a
rapid test at the airport immediately before departure (given many
infected may have started shedding the virus in the previous 72
hours and most, but not all, of such cases will be detected by a rapid
test even though it has lower sensitivity). Of note is that such
arrangements are considered legally acceptable (see the above row).
Pre-departure quarantine (eg, for a week), would provide additional
Top priority
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

Policy option Description
Our priority
rankings
assurance, but this would probably need to be in a transport hub (eg,
at an airport hotel at Singapore or Hawaii) where NZ and Australian
officials were permitted access to ensure quality processes. Even if
establishing a formal facility is shown to be impractical, all
incoming travellers could be asked to self-quarantine as strictly as
possible in the week before travel, eg, by a request through the
passenger booking system (see Policy Option 4).
3. Pre-departure
vaccination
Make travel contingent on completing a course of approved
vaccination. This measure assumes the vaccine is at least partially
effective at preventing transmission. This requirement needs further
investigation and development.
Uncertain
4. Use passenger
booking systems to
reduce infection
risk
Require passengers to declare pre-departure COVID-19 precautions
via the system that they use to book spaces in quarantine facilities
prior to travel. Such a system is operating in NZ and could be
adopted more widely in Australia.
High priority
5. Increase in-flight
precautions
Explore means to reduce the risk of in-flight infection as
documented on a flight to NZ.
24
This could be via more stringent
enforcement of mask wearing in airports and on flights, use of
higher-efficacy masks (and/or double masking), and minimizing
talking when masks are displaced during eating and drinking on
flights. Improved ventilation and spacing requirements on flights
might also be worthwhile.
High priority
6. Reduce infection
risk at airports and
transit hubs
Ensure measures are in place at departure airports and transit hubs
to minimize the risk of cross infection (eg, through physical
distancing and mask use).
Medium
priority
7. Improve local
transport
arrangements
Ensure sufficient physical distancing of travellers on arrival and in
transit to quarantine (eg, lowering density on buses). For such
arrangements, N95 masks could be required.
Medium
priority
8. Shift to discrete
quarantine units
Shift some or all quarantine facilities to rural military bases or
camps where discrete units (eg, mobile homes or caravans) could be
appropriately spatially separated. The success (to date – see Table
A1 in the Appendix) of the Howard Springs facility (a converted
workers’ camp
12
) should be considered. This approach allows for
natural ventilation and eliminates shared indoor spaces. If spaces
were limited, then these settings could be used for travellers from
the highest risk countries.
High priority
9. Restrict hotel
quarantine in large
cities to low-risk
travellers
Reserve hotel quarantine in large cities to the lowest risk category
of travellers, with hotels in more minor cities being used for the
highest risk category of travellers. However, the risk/benefit
analysis of such changes would need to consider airport access and
if the additional travelling to minor cities poses excessive additional
risk.
High priority
10. Expand use of
PCR testing of
saliva in facility
workers (and
travellers)
Expand the regular (daily) use of PCR testing of saliva of facility
workers to all facilities in both countries. This approach could also
be considered for all travellers, albeit potentially still combined
with existing testing regimens. In view of increased transmissibility
of new variants, consideration should be given to testing of all
workers in border-associated occupations (eg, providing airline
meals and laundry services) at least twice per week. Documented
negative tests at appropriate frequency should be an occupational
requirement for all border workers instead of the self-report systems
High priority
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

Policy option Description
Our priority
rankings
(as currently used in NZ).
11. Accelerate or
mandate
vaccination for
quarantine staff
Vaccinate all quarantine workers against COVID-19 and redeploy
all unvaccinated workers. This measure will be particularly valuable
when vaccines are known to prevent transmission in addition to
protecting recipients from illness.
As of April
2021, this is
measure is
nearing
completion in
some
jurisdictions
12. Cohorting
complete flights of
travellers
Cohorting of flights means that all returnees arriving into a country
go to the same quarantine facility until that facility is full and then
the intake switches to another facility and so on. This approach is
designed to reduce cross-infection in such facilities. This system
was introduced in NZ on 16 May 2021.
Medium
priority
13. Upgrade
processes at
quarantine facilities
Upgrade processes at quarantine facilities in terms of eliminating
shared spaces (eg, no shared exercise areas and shared smoking
areas), in particular ensuring that day cohorts do not mix under any
circumstances. Ventilation improvements could also be considered
with limiting the use of rooms to those with external windows.
Medium
priority
14. Prosecute rule
breaking in
quarantine facilities
Enforce quarantine facility rules more rigorously. Rule breaking,
which is relatively common in NZ facilities,
25
could start to be
prosecuted (given no prosecutions during 2020).
Medium
priority
15. Improve
conditions for
quarantine staff
Improve working conditions for the staff in quarantine facilities to
minimize the risk of overwork (which may increase the risk of PPE
failures) or of workers taking on other part-time jobs in other
settings. For example, in February 2021 there were still concerns by
NZ health workers about staffing inadequacies in these facilities.
High priority
16. Improve
management of
travellers who
smoke
Introduce specific measures for travellers who are nicotine
dependent to reduce their need to smoke in designated areas during
their travel and while in managed quarantine (eg, nicotine
replacement treatment as a requirement for travel).
Medium
priority
17. Add post-
quarantine control
measures
Introduce a post-quarantine period of home-quarantine to reduce the
risk of local transmission arising from undetected infections in
people leaving hotel quarantine facilities (which may arise from
either exceptionally long incubation periods or cross infection
during quarantine stays). Post-quarantine testing could also be used
to detect such infections.
Medium
priority
18. Mandate the
use of digital
contact tracing
tools
Mandate quarantine workers to use digital technologies (eg, the
Bluetooth function on the NZ COVID Tracer smartphone app) to
facilitate contact tracing in the event of a border failure. Travellers
could be required to use such technologies for two weeks after
completing their time in quarantine. There is also a case for
travellers using these tools within quarantine as (at least in NZ)
quarantine facilities are sometimes evacuated for fire alarms and
burst water pipes.
Medium
priority
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

Conclusions
In summary, Australia and New Zealand have had 24 COVID-19 identified failures arising
from quarantine systems up to 31 March 2021. Quarantine system failures can be costly in
terms of lives and economic impacts such as lockdowns. Ongoing improvements or
alternatives to hotel-based quarantine are required.
Competing interests: Nil.
Funding: Prof Baker and Dr Kvalsvig received funding support from the Health Research
Council of New Zealand (20/1066). Dr Grout, Ms Katar, Dr Ait Ouakrim, Dr Summers, Prof
Blakely, and Prof Wilson did not have external funding support.
Appendix
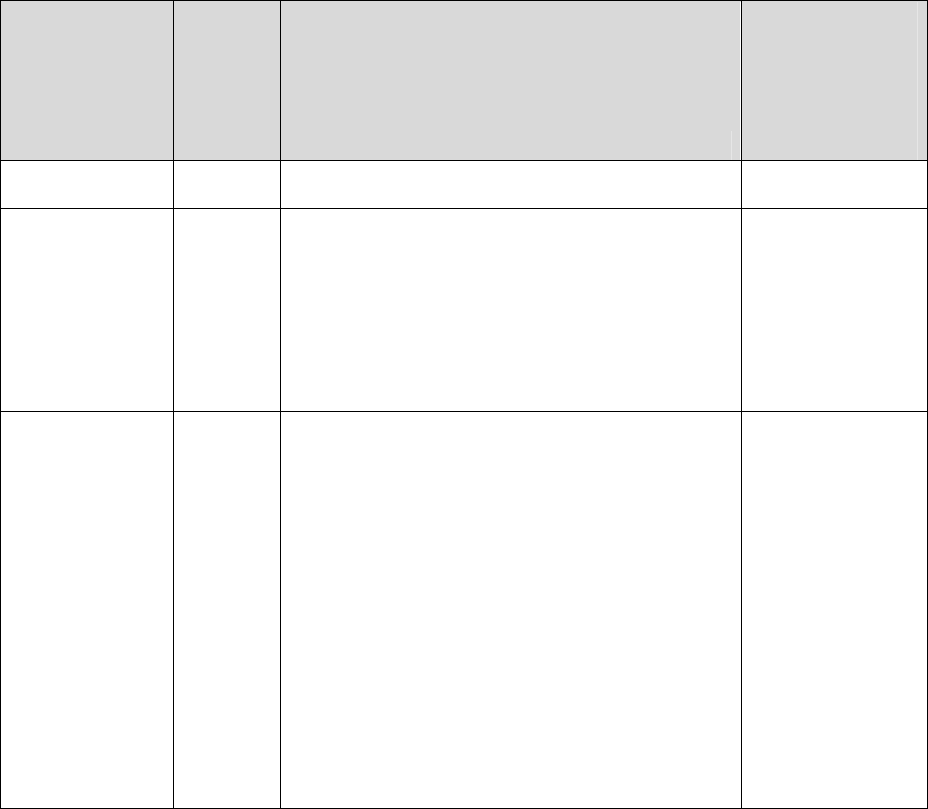
Appendix Table A1: List of COVID-19 border control failures associated with quarantine
systems in Australia and New Zealand during 2020 and up to 31 March 2021
Event
Extent of
known
spread
Details
Event preventable
with full
vaccination of
frontline border
workers
(assuming 100%
effectiveness)?
Australia
Rydges Hotel –
Victoria "second
wave" outbreak
(late May to late
October 2020)
Over
19,800
cases,
26 27
and over
800
deaths
28
Genomic testing indicated that 99% of Victoria's
second wave of community COVID-19 cases were
linked to transmission events related to returned
travellers infecting workers at the Rydges Hotel in
Carlton and the Stamford Plaza Hotel (see row
below) in Melbourne's central business district
(CBD), which were used as facilities for quarantine.
29
Specifically, around 90% of cases can be traced
back to a single family of four that returned to
Australia in mid-May and were quarantined at the
Rydges Hotel.
30
The virus then spread from the
infected workers to the community, with high rates of
local transmission.
29
The outbreak led to a stringent
lockdown for 112 days in the state, with particularly
strict measures in the major city of Melbourne.
31
At
least nine people employed in Melbourne's hotel
quarantine program tested positive between late July
and early October 2020, although the cases may
have been a reflection of substantial community
transmission in Melbourne at the time rather than
additional hotel quarantine failures.
32
Two of those
cases worked while infectious.
32
Likely
Stamford Plaza
Hotel - Victoria
"second wave"
outbreak (late
May to late
See row
above
Almost 10% of cases in Victoria's "second wave"
outbreak were attributable to an outbreak at the
Stamford Hotel in mid-June.
29
The outbreak was
traced back to international travellers who returned
to Australia in early June,
29
and then was spread by
Likely
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

Event
Extent of
known
spread
Details
Event preventable
with full
vaccination of
frontline border
workers
(assuming 100%
effectiveness)?
October 2020)
security guards who worked at the facility
.
33
Marriot Hotel at
Circular Quay in
Sydney, New
South Wales
[NSW] (August
2020)
2 security
guards
A security guard at the Marriot Hotel at Circular
Quay in Sydney tested positive for COVID-19 on 15
August.
34
Genomic sequencing linked the infection
to a returned overseas traveller at the facility.
34
A
second security guard subsequently tested
positive.
35
Likely
Parafield outbreak
in South Australia
(December 2020)
33
cases
28
Genomic testing indicated that Adelaide's Parafield
cluster was linked to transmission events related to a
returned traveller in a quarantine hotel infecting
workers in the facility, possibly due to poor
ventilation at the facility.
29
The virus spread from the
workers to the community, resulting in a strict
lockdown.
29
Likely
Quarantine hotel
facility cleaner
infected in
Sydney, NSW
(December 2020)
A single
worker
A quarantine hotel worker (a cleaner) who
completed shifts at two quarantine hotels, the Ibis
Hotel and the Novotel in Darling Harbour in Sydney,
tested positive in early December.
36
There was also
spread in a facility with 5 returned travellers being
infected.
Likely
Avalon outbreak
in NSW (January
2021)
151 cases
(as of 11
January
2021)
37
It has been reported that genomic sequencing
suggests that the strain is of US origin and entered
Australia via an infectious returned traveller who
entered hotel quarantine upon arrival.
36
It is currently
unknown how the virus spread to the community and
source investigations were still underway (as per
January 2021). Case numbers include those from
the linked Croydon and Wollongong clusters, but not
the linked Black Rock cluster in Victoria (27 cases as
of 5 January 2021) due to separate reporting by
states.
Unclear
Berala outbreak in
NSW (January
2021)
26 cases
(as of 11
January
2021)
37
It has been reported that genomic sequencing linked
the outbreak back to infectious international
travellers.
38
A patient transport worker transferred
infectious travellers from Sydney Airport to a
hospital.
37 38
Another patient transport worker who
was a close contact of the first then also tested
positive
37 38
The virus then spread from the second
infected worker into the community, seeding the
Berala outbreak.
38
Likely
Hotel Grand
Chancellor
outbreak in
Brisbane,
Queensland
(January 2021)
6 cases
(as of 13
January
2021)
39
A hotel quarantine worker in Brisbane tested positive
in early January 2021 for the UK variant of COVID-
19 (ie, B.1.1.7).
40
This case led to a three-day
lockdown in the greater Brisbane area, while contact
tracers worked to ensure there was no community
transmission of the strain.
41
It was later revealed that
there were six genomically linked cases within the
quarantine facility, including the hotel quarantine
worker and five returned travellers.
39
Likely
Four Points by A single A Perth quarantine hotel security guard, who worked
Likely
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

Event
Extent of
known
spread
Details
Event preventable
with full
vaccination of
frontline border
workers
(assuming 100%
effectiveness)?
Sheraton
hotel,
Western Australia
(January 2021)
worker
a second job as a ride share driver, tested positive to
the UK strain of SARS-CoV-2, sparking a five-day
lockdown for 80 per cent of the state's population, in
an attempt to stop any further transmission.
42
It’s
believed he was exposed to the virus on the 26
January when he worked at Four Points by
Sheraton, on the same floor where a quarantined
returned traveller with a confirmed case of the UK
variant was staying. After feeling sick on 28 January,
the case visited a GP, and tested positive on 30
January. The exact cause is unknown, but it’s
believed poor ventilation could be a factor.
43
This
comes a week after Western Australia committed to
daily testing of the hotel quarantine staff, instead of
weekly.
44
Quarantine hotel staff, including cleaners,
security guards and catering staff, are no longer
allowed to have second jobs but will receive a pay
increase of about 40 per cent as compensation.
42
It
has been announced an inquiry will be held.
43
Grand Hyatt
Hotel, Victoria
(February 2021)
A single
worker
One 26-year-old staff member at the Grand Hyatt
Hotel (an isolation facility) tested positive for the
highly transmissible UK variant of COVID-19 (ie, the
B.1.1.7 variant) in February 2021, leading to
heightened restrictions.
45
The close contacts of the
case all tested negative, and the outbreak did not
spread into the wider community.
45
Likely
Holiday Inn Hotel
Cluster, Victoria
(February 2021)
22 cases
Twenty-two cases have been linked to the Holiday
Inn cluster in Melbourne, where an infected returned
traveller used a nebuliser, causing an outbreak and
a 5-day lockdown.
46
There were no further cases
detected in the community during the lockdown as
all confirmed cases had already been informed of
their status as close contacts and were in isolation
for the duration of their infectious period. Cases
included returned travellers, hotel quarantine staff
and their families, as well as a Melbourne Airport
worker.
46
Likely
Princess
Alexandra
Hospital Doctor
outbreak,
Brisbane (March
2021)
6 cases
47
A doctor and a nurse (see row below) who worked at
the Princess Alexandra Hospital while unvaccinated
were linked to two separate COVID-19 outbreaks.
47
While both outbreaks were the highly transmissible
UK variant of the disease and originated at the same
hospital, they were from two different sources.
47
The
doctor tested positive on 12 March 2021, with
subsequent infections in 5 other persons.
47
These
outbreaks resulted in a 3-day lockdown just before
the Easter holiday.
47
Likely (we
considered health
workers at the
Princess Alexandra
to be “border
workers” given that
the hospital
patients were still
part of the
quarantine system)
Princess
Alexandra
Hospital Nurse
outbreak,
13
cases
48
A nurse (see row above) who worked on a COVID-
19 ward at the Princess Alexandra Hospital while
unvaccinated tested positive in late March.
47
Genome sequencing links the case to an overseas
Likely (we
considered health
workers at the
Princess Alexandra
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

Event
Extent of
known
spread
Details
Event preventable
with full
vaccination of
frontline border
workers
(assuming 100%
effectiveness)?
Brisbane (March
2021)
traveller from India who was being cared for at the
hospital.
49
The nurse's sister, a number of attendees
at a “hen's party”, and several other contacts were
subsequently infected.
47
to be “border
workers” given that
the hospital
patients were still
part of the
quarantine system)
Sofitel Wentworth
Hotel in Sydney,
NSW (March
2021)
A single
security
guard
A security guard at the Sofitel Wentworth in Sydney
tested positive for COVID-19 on 13 March through
routine surveillance testing.
50
Genomic sequencing
linked the case to a returned traveller and
subsequent testing revealed that another returned
traveller was also infected within the facility.
50
Likely
New Zealand
Auckland August
2020 outbreak
A total of
179
cases,
with 3
deaths
51
The cause of this outbreak remains unknown, but
genomic work probably provides the best evidence
to this being a border facility (isolation or quarantine
facility) failure: “There are a large number of similar
genomes which are from the UK, which would seem
to suggest the UK is the most likely source of any
unknown importation”.
52
This was at a time when
40% of cases in NZ quarantine/isolation facilities did
not have genomic work on the virus infecting them
(ie, there was not enough complete virus in the
samples). It was also estimated
52
that there was only
a very tiny risk of this outbreak being a continuation
of the March/April spread of the pandemic in NZ:
“Our Bayesian phylogenetic analysis … estimates
that there is a 0.4% probability that case 20VR2563
is in the “sister clade”' of the Auckland cluster.”
Finally, the chance of the outbreak being from
contaminated imported food was also considered
very unlikely: “Our Bayesian phylogenetic analysis
… shows that the estimated mutation rate on the
branch leading to the cluster is not a lot smaller than
elsewhere in the tree, lending little weight to the
possibility that the virus lay dormant on packing
material for a long period of time.”
Unclear
Border facility
maintenance
worker infected
(August 2020)
A single
worker
A shared lift environment in a quarantine hotel (the
Rydges Hotel in Central Auckland was the source
suspected by officials,
53
with the sharing being only
minutes apart.
52
The genomic sequencing indicated
the same virus infecting the worker as per a recent
traveller in the same facility.
52
Likely
Border facility
health worker
infected
(September 2020)
A single
worker
This was a work-related infection associated with a
hotel facility used for isolating infected cases (the Jet
Park Hotel, Auckland), given that the case was
linked via genomic sequencing to 3 cases within the
facility.
54
Some details of the full investigation report
were provided to the media and these suggested
that while the nurse wore personal protective
equipment (PPE), there was a period where the
Likely
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

Event
Extent of
known
spread
Details
Event preventable
with full
vaccination of
frontline border
workers
(assuming 100%
effectiveness)?
associated patient did not have a mask on during
treatment.
55
This situation could have contributed to
a failure of the PPE worn by the nurse.
Traveller-related
outbreak /
Christchurch
border facility
(September 2020)
The
traveller
and 2
others
(total of 3
cases)
This person was thought to have been infected
within a hotel quarantine facility before then moving
into the community, according to the Ministry of
Health.
56
This infected traveller appears to have then
infected another person (the Ministry suggest this
may have occurred on a charter flight after leaving
the facility).
56
A household contact was also reported
as becoming infected.
57
No
Border facility
health worker
(Case A) in
Christchurch (Nov
ember 2020)
A single
worker
This was a work-related infection associated with a
facility used for isolating infected cases. Both this
case (and “Case B” below) had the virus genome
sequencing linked to infection in a group of
international mariners in the same hotel facility but
with different virus subtypes in each case.
53
“The
finding supports the current theory that there were
two separate events infecting both workers at the
facility.” These cases of infected health workers
appear to have contributed to border control nurses
threatening strike action if they were not supplied
with improved PPE.
27
One estimate was that 12 of
the mariners were infected on arrival in NZ, but with
subsequent spread within the facility a total of 31
mariners were ultimately infected.
58
Likely
Another border
facility health
worker (Case B)
(see above)
A single
worker
This was a separate work-related infection
associated with a border control facility – see in the
row above.
Likely
Defence Force
worker outbreak
(November 2020)
The
worker, a
co-worker
and 4
others
(total of 6
cases)
This was a work-related infection in a Defence Force
worker associated with a hotel border facility in
Auckland (used for isolating known infected cases).
“The genome sequencing we have conducted on
Case A’s test result shows a direct link to two
travellers who are part of a family group in the
quarantine facility”.
59
The route of transmission to
one of the community cases remains a mystery
(albeit they worked in the same locality within
Auckland City). Associated with these cases, the
Prime Minister made statements around the need for
further risk reduction.
60
Likely
Traveller
infectious after
leaving a
quarantine facility
(January 2021)
1 traveller
A traveller was identified as being infectious in the
community after leaving a quarantine facility
(Pullman, Auckland). The traveller reportedly had the
South African variant (lineage B.1.351) of the
pandemic virus.
61
Genome sequencing has linked
this case to another traveller who was in the same
facility.
62
The transmission mechanism has not been
precisely identified with investigations still
proceeding as of mid-February 2021. However,
No
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint
Event
Extent of
known
spread
Details
Event preventable
with full
vaccination of
frontline border
workers
(assuming 100%
effectiveness)?
officials consider it likely to have been a separate
transmission event to the one in the following row.
Travelers
infectious after
leaving a
quarantine facility
(January 2021)
2
travellers
and a
contact
Two travellers (a parent and child) were identified as
infectious in the community after being infected with
the South African variant (lineage B.1.351), of the
pandemic virus with a link to a quarantine facility
(Pullman, Auckland).
63
A close contact (the mother
of the child) also became infected.
64
The
transmission mechanism has not been precisely
identified with investigations still proceeding as of
mid-February 2021.
No
MIQ workers
(March 2021)
3 workers
A cleaner at the Grand Millennium Hotel MIQ facility
in Auckland (Case A) tested positive during routine
surveillance testing on 22 March 2021.
65
While a
household contact returned a weak positive the next
day,
66
subsequent tests were negative.
67
The MIQ
worker had recently been vaccinated (with the
Pfizer/BioNTech vaccine) on 23 February, with a
second dose on 16 March,
66
although they tested
positive before full protection from the vaccine could
be expected. Their family had not yet been
vaccinated.
66
Genome sequencing revealed that
Case A was infected with the highly transmissible
variant first identified in the UK (B.1.1.7) and was
linked to a traveller in the facility who had arrived on
13 March.
68
In early April, two unvaccinated security
guards at the same facility tested positive (Cases B
and C) and genome sequencing linked the two
cases to Case A.
69 70
Likely
Approaches to managing quarantine in Australia and New Zealand
Table A2 details the various approaches to quarantine used in both countries. Key features of
which are summarised below:
• The length of quarantine in all jurisdictions is 14 days.
• Almost all jurisdictions require at least two separate PCR tests for travellers: one
shortly after arrival and another closer to the end of the quarantine period.
• Many jurisdictions have introduced or are considering additional tests for travellers,
either earlier in (eg, Day 0/1 in New Zealand) or after (eg, Day 16 in New South
Wales) the quarantine period. This is in response to concerns about new highly
infectious variants in early 2021.
• Australia does not currently have a national strategy for quarantine.
• Detailed information on quarantine programs for each Australian state/territory is
limited and in many cases we had to rely on news articles for additional details in
compiling Table A2. Descriptions of PPE required for quarantine staff in different
jurisdictions were particularly difficult to identify and information often was not
available by staff role (eg, security guards vs cleaners).
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

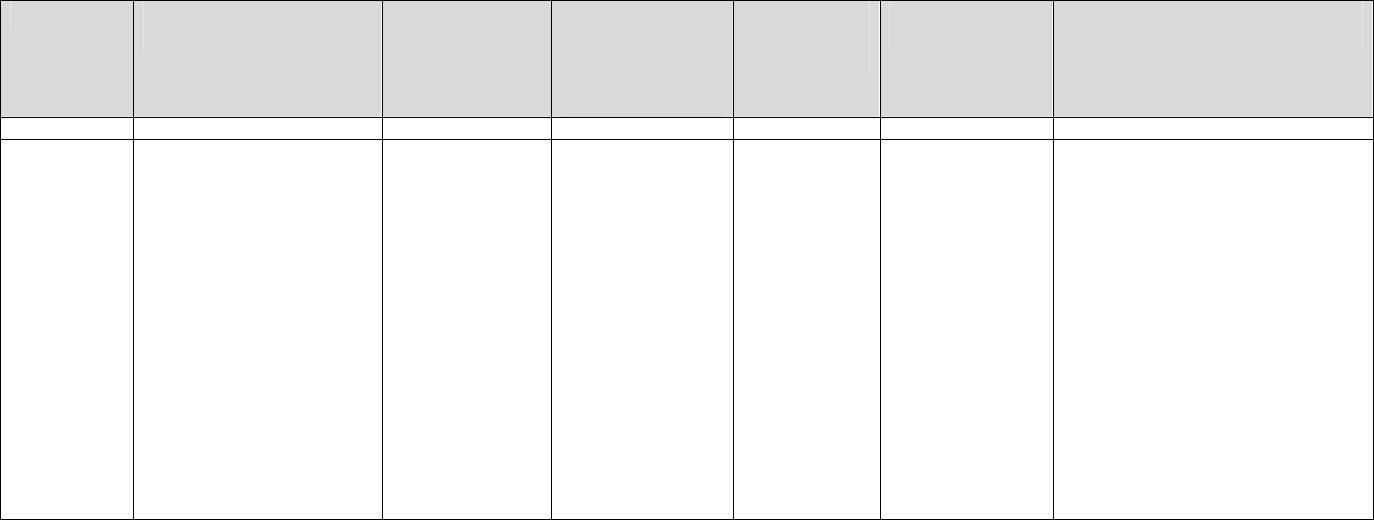
Appendix Table A2: Description of key infection control processes and surveillance at quarantine facilities in Australia and New Zealand as of 31
March 2021 (with the length of quarantine being 14 days in all jurisdictions)
Jurisdiction
PCR testing regimen for
travellers
PCR testing
regimen for staff
Mask
requirements for
travellers
(outside of
rooms)
Mask
requirements
for staff
Shared space
restrictions
Comments and historical
changes of note
New Zealand
(NZ)
NZ requires evidence (with
some exemptions) before
boarding of an aircraft to
NZ from most international
locations of a COVID-19
pre-test of either a PCR
(including RT-PCR), LAMP
or antigen test taken 72
hours before scheduled
departure (introduced
between 15 and 25
January 2021).
71
NZ
requires tests on days: 0/1
(most), 3 and 12.
72
Weekly
(nasopharyngeal
swab) for some
staff,
72
but with
selected
voluntary use of
daily saliva
(PCR) testing in
selected
locations. Staff
transporting
travellers to
hotels are also
subject to
testing.
72
It is
possible that the
required testing
has not been fully
undertaken in
some
instances.
73
Single-use face
masks are
provided to
travellers and are
to be used when
outside of room.
72
They are required
to be worn if
someone enters a
hotel room, such
as during testing.
Surgical or
procedure
masks to be
worn by staff if
nearby
travellers.
74
N95/P2 masks
to be worn by
staff when 2
meters
physical
distancing
cannot been
maintained by
staff when
nearby
confirmed or
probable
cases of
COVID-19
(effective 26
November
2020).
75
There are some
restrictions, with
travellers in some
facilities required
to book allocated
times to access
shared spaces –
but there remain
shared
recreational,
exercise, and
smoking areas in
most facilities.
72
The testing process has changed
over time with a day 0/1 test
introduced in January 2021 for
travellers from most countries
(excluding those from some low-
risk countries). On some occasions
the infection control processes in
the facilities were found to be
suboptimal (eg, 19 mariners
infected while in one facility
58
).
Some facilities run daily bus trips to
take travellers to outdoor exercise
areas, a practice which has raised
concerns from epidemiologists.
Vaccination of staff was initially not
required, however, if staff are not
vaccinated, they will be redeployed
to a non-frontline role.
76 77
Australian States and Territories
Australia requires evidence (with some exemptions) for boarding aircraft to Australia from most international locations of a negative COVID-19 PCR test taken 72
hours or less before scheduled departure (introduced on 22 January 2021).
78
Australian
Capital
Territory
ACT requires tests
between days 0-2 and
between days 12-13.
79
Asymptomatic
staff to be tested
every 7 days.
79 80
Masks must be
worn when
opening hotel
Possible
surgical mask
use (as
Travelers are
required to remain
within their hotel
To date, ACT has only accepted
repatriation flights.
81
All front-line quarantine workers are
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

Jurisdiction
PCR testing regimen for
travellers
PCR testing
regimen for staff
Mask
requirements for
travellers
(outside of
rooms)
Mask
requirements
for staff
Shared space
restrictions
Comments and historical
changes of note
(ACT)
doors
.
79
If sharing
a hotel room and
COVID-19
symptoms
develop, a face
mask must be
worn inside the
hotel room.
79
suggested by
photographic
evidence).
81
room
.
79
required to be vaccinated for
COVID-19 as a condition of
employment (policy announced in
late March 2021).
82
Queensland
Tests required on days 2
and 11.
83
Staff are required
to have throat &
nasal swabs or a
saliva test within
7 days after
commencing
work at a facility,
and then daily
saliva testing,
with rolling throat
& nasal swabs
every 7 days.
84
Travelers are
required to wear a
face mask when
traveling to a
quarantine hotel
until reaching the
hotel room.
85
Travelers are also
requested to wear
marks where
appropriate.
86
Staff are
required to
wear PPE
(including a
surgical
mask
86
) when
entering a
traveller’s
room to
conduct
COVID-19
tests.
87
Travelers have no
access to shared
facilities and are
required to remain
within their
allocated room.
87
Testing clinicians ‘may’ ask
travellers to wear ‘appropriate PPE’
when being tested for COVID-19.
87
Testing clinicians are advised not to
enter a traveller’s room unless
there is no other way to collect
specimen.
86
Staff who working
within direct or indirect contact are
required to be vaccinated.
88
New South
Wales
(NSW)
Tests required on days 2
and 12.
89
PCR or saliva
collection: Hotel
staff in
quarantine facility
(effective 14
December 2020)
and persons
providing security
services to
quarantine facility
(effective 11
January 2021);
Travelers are
typically not
allowed outside of
rooms.
92
Additional
information was
not available on
mask requirements
for travellers.
PPE (including
a surgical
mask) when
conducting
COVID-19
test,
93
cleaning
rooms,
94
or
transferring
travellers and
their
luggage.
95
No smoking, e-
cigarette use, or
outside exercise
allowed while in
hotel
quarantine.
89 92
In February 2021, NSW introduced
a test for travellers on day 16.
37
Saliva swabs are also required from
the following designated quarantine
facility workers once per shift, taken
during shift: NSW Police Officers
(effective 20 January 2021), and
Healthcare staff providing medical
treatment or care to a person
(effective 18 January 2021).
90
Quarantine transport workers
(effective 21 January 2021)
96
and
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

Jurisdiction
PCR testing regimen for
travellers
PCR testing
regimen for staff
Mask
requirements for
travellers
(outside of
rooms)
Mask
requirements
for staff
Shared space
restrictions
Comments and historical
changes of note
testing taken
once per shift,
during shift.
90 91
designated airport workers also
receive daily saliva testing.
91
Vaccination is not currently
compulsory for staff.
97
Northern
Territory
At the Howards Springs
quarantine facility travellers
are tested upon arrival.
98
It
remains unclear how many
other COVID-19 tests are
required and when.
Daily testing
(nasal swab) of
staff at Howards
Springs
quarantine
facility.
99 100
Masks provided to
travellers, and
must be worn
when on veranda
of allocated room,
and when opening
door of room, or
going outside of
room.
101
Staff are
required to
wear PPE
(including a
surgical mask)
when
interacting with
travellers, and
are also
required to be
photographed
in their PPE
before starting
a shift.
99
There are
balconies
attached to each
traveller’s cabin
for individual use,
and also used
during COVID-19
testing at the
Howard Springs
quarantine
facility.
100
However, it is
unclear whether
reports of use of a
swimming pool
are correct.
98
Managed quarantine is not
undertaken in hotels and is closer
to ideal in terms of ventilation and
reduced shared space: ‘In Darwin,
rooms are single accommodation,
with no internal connecting doors
between the rooms. In Alice
Springs families are accommodated
in shared rooms, based on room
availability at the time.
101
' In some
managed supervised quarantine
locations, they do not allow for
delivery services.
101
Movement of
staff within the Howards Springs
quarantine facility is restricted.
99
Staff buddy systems are in place,
and careful monitoring of PPE use
with photographs of PPE taken
before each shift at Howards
Springs quarantine facility.
100
Vaccination of staff began in late
February 2021.
102
South
Australia
Tests are required on days
0, 5, and 13.
103
Staff are required
to have nose and
throat swabs
once every 8
days.
104 105
Masks must be
worn when
opening hotel
doors.
103
Returned
travellers are only
allowed to leave
their rooms in an
‘Hotel staff
must wear
appropriate
PPE and
maintain at
least 1.5
meters
Travelers must
remain within their
hotel room.
103
A requirement for a day 16 test for
travellers after leaving hotel
quarantine may be introduced in
February 2021.
107
Additionally, as
of 8 February 2021, hotel
quarantine workers were required
to have daily saliva tests.
107
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

Jurisdiction
PCR testing regimen for
travellers
PCR testing
regimen for staff
Mask
requirements for
travellers
(outside of
rooms)
Mask
requirements
for staff
Shared space
restrictions
Comments and historical
changes of note
emergency
situation.
distance from
guests at all
times’.
106
Vaccination of staff is not
compulsory (current as of February
2021).
108
Tasmania
Tests are required within
48 hours of entering
quarantine and after day
10 of the quarantine
period.
109
Staff must get
tested every 5 to
8 days after their
first shift, then
tested every 5 to
8 days, until 14
days after their
last shift.
110
Required to wear a
facemask when
travelling to
quarantine hotel
and if leaving the
hotel room for an
approved purpose
(such as seeking
medical care) a
face mask must be
worn at all times
(unless an
exemption
applies).
109
Transport,
security, and
health officials
involved in
hotel
quarantine will
have
'appropriate
PPE'.
111
Travelers must
remain within their
hotel room.
109
Hotel quarantine workers given
wage supplements to prevent them
taking second jobs in effort to
reduce risk of COVID-19
transmission – December 2020.
112
Workers at government-designated
quarantine sites must undertake
saliva screening once per shift.
110
Vaccination of staff is prioritized in
Tasmania, and currently not
compulsory.
113
Victoria
Tests are required within
24 hours of arrival in
Victoria, as well as on (or
about) days 4, 12 and
14.
114
Daily testing is
required for staff
(even on days
off).
21 115
Travelers are not
allowed to leave
their rooms unless
there is an
emergency.
21
Travelers must
wear masks when
opening the doors
to collect their
food.
Full PPE is
required for
staff while on
shift.
There are no
shared spaces;
returned travellers
must remain in
their rooms.
21
After the significant failure that led
to over 19,800 cases, and over 800
deaths, Victoria began welcoming
returned travellers in December
with a revamped hotel quarantine
system which included a number of
improvements, such as daily testing
of staff, voluntary regular testing of
family members of staff, advanced
contact tracing, a ban on secondary
face-to-face employment for key
staff, strengthened PPE protocols,
and dedicated 'health hotels' for
positive and suspected cases and
their close contacts.
21
All front-line
staff were to be vaccinated with first
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint
Jurisdiction
PCR testing regimen for
travellers
PCR testing
regimen for staff
Mask
requirements for
travellers
(outside of
rooms)
Mask
requirements
for staff
Shared space
restrictions
Comments and historical
changes of note
dose by early April
.
116
Western
Australia
Tests are required within
24 hours of arrival and
again on day 12.
117
Staff must
undergo a nose &
throat PCR test
every 7 days
along with a daily
self-collected
mouth swab PCR
test, effective
from 31 January
2021.
118
Travellers are
required to wear
masks when
opening hotel room
door (must be put
on 2 minutes
before opening
door).
119
Travelers
must remain in
their rooms.
Hotel
quarantine
security staff in
Perth were not
required to
wear masks
up to early
February
2021,
120
however
masks and
eye protection
are now
required (from
late February
2021).
121
Individuals in
quarantine are
required to remain
in their hotel
room; any
exercise must be
done inside the
hotel room and no
smoking is
allowed in
hotels.
117
Previous PCR testing from 8
January 2021 for staff only required
testing every 7 days and no daily
mouth swab.
118
Certain hotel
quarantine workers, including
security guards, cleaners, and
catering staff, have been given a
40% wage increase and are no
longer allowed to hold a second
job.
42
There are possible plans to
make vaccination compulsory for
staff.
122
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

References
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint
. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint

. CC-BY-NC-ND 4.0 International licenseIt is made available under a
is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. (which was not certified by peer review)
The copyright holder for this preprint this version posted April 30, 2021. ; https://doi.org/10.1101/2021.02.17.21251946doi: medRxiv preprint
