
1Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
2023
O ur Epidemic
of Loneliness
and Isolation
The U.S. Surgeon General’s Advisory on the
Healing Effects of Social Connection and Community

2Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Table of Contents
Letter from the Surgeon General 4
About the Advisory 6
Glossary 7
Introduction: Why Social Connection Matters 8
What is Social Connection? 10
Current Trends: Is Social Connection Declining? 12
Trends in Social Networks and Social Participation 13
Demographic Trends 15
Trends in Community Involvement 16
What Leads Us to Be More or Less Socially Connected? 16
Groups at Highest Risk for Social Disconnection 19
Impacts of Technology on Social Connection 19
Risk and Resilience Can Be Reinforcing 21
Call Out Box: Lessons from the COVID-19 Pandemic 22
Individual He
alth Outcomes 24
Survival and Mortality 24
Cardiovascular Disease 26
Hypertension 26
Diabetes 27
Infectious Diseases 28
Cognitive Function 28
Depression and Anxiety 29
Suicidality and Self-Harm 29
Social Connection Influences Health Through Multiple Pathways 30
Social Connection Influences Biological Processes 32
Social Connection Influences Psychological Processes 33
Social Connection Influences Behaviors 34
Individual Educational and Economic Benefits 34
Educational Benefits 34
Economic Benefits 35
Chapter 1
Overview
8
Chapter 2
How Social Connection
Impacts Individual
Health and Well-Being
23

3Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Socially Connected Communities 37
The Benefits of More Connected Communities 39
Population Health 39
Natural Hazard Preparation and Resilience 40
Community Safety 41
Economic Prosperity 41
Civic Engagement and Representative Government 42
The Potential Negative Side of Social Connection 43
Societal Polarization 44
The Six Pillars to Advance Social Connection 47
Pillar 1: Strengthen Social Infrastructure in Local Communities 48
Pillar 2: Enact Pro-Connection Public Policies 49
Pillar 3: Mobilize the Health Sector 50
Pillar 4: Reform Digital Environments 51
Pillar 5: Deepen our Knowledge 52
Pillar 6: Cultivate a Culture of Connection 53
Recommendations for Stakeholders to Advance Social Connection 54
National, Territory, State, Local, and Tribal Governments 55
Health Workers, Health Care Systems, and Insurers 56
Public Health Professionals and Public Health Departments 57
Researchers and Research Institutions 58
Philanthropy 59
Schools and Education Departments 60
Workplaces 61
Community-Based Organizations 62
Technology Companies 63
Media and Entertainment Industries 64
Parents and Caregivers 65
Individuals 66
Strengths and Limitations of the Evidence 67
Acknowledgments 69
References 72
Chapter 3
How Social Connection
Impacts Communities
36
Chapter 4
A National Strategy
to Advance
Social Connection
45
TABLE OF CONTENTS

4Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
When I first took office as Surgeon General in 2014, I didn’t view
loneliness as a public health concern. But that was before I embarked
on a cross-country listening tour, where I heard stories from my fellow
Americans that surprised me.
People began to tell me they felt isolated, invisible, and insignificant.
Even when they couldn’t put their finger on the word “lonely,” time and
time again, people of all ages and socioeconomic backgrounds, from
every corner of the country, would tell me, “I have to shoulder all of life’s
burdens by myself,” or “if I disappear tomorrow, no one will even notice.”
It was a lightbulb moment for me: social disconnection was far more
common than I had realized.
In the scientific literature, I found confirmation of what I was hearing.
In recent years, about one-in-two adults in America reported experiencing
loneliness.
1-3
And that was before the COVID-19 pandemic cut off so
many of us from friends, loved ones, and support systems, exacerbating
loneliness and isolation.
Loneliness is far more than just a bad feeling—it harms both individual
and societal health. It is associated with a greater risk of cardiovascular
disease, dementia, stroke, depression, anxiety, and premature death.
The mortality impact of being socially disconnected is similar to that
caused by smoking up to 15 cigarettes a day,
4
and even greater than
that associated with obesity and physical inactivity. And the harmful
consequences of a society that lacks social connection can be felt in
our schools, workplaces, and civic organizations, where performance,
productivity, and engagement are diminished.
Given the profound consequences of loneliness and isolation, we have
an opportunity, and an obligation, to make the same investments in
addressing social connection that we have made in addressing tobacco
use, obesity, and the addiction crisis. This Surgeon General’s Advisory
shows us how to build more connected lives and a more connected society.
If we fail to do so, we will pay an ever-increasing price in the form of our
individual and collective health and well-being. And we will continue
to splinter and divide until we can no longer stand as a community or
a country. Instead of coming together to take on the great challenges
before us, we will further retreat to our corners—angry, sick, and alone.
Letter from the Surgeon General
Dr. Vivek H. Murthy
19th and 21st Surgeon General
of the United States

5Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
We are called to build a movement to mend the social fabric of our nation.
It will take all of us—individuals and families, schools and workplaces,
health care and public health systems, technology companies,
governments, faith organizations, and communities—working together to
destigmatize loneliness and change our cultural and policy response to it.
It will require reimagining the structures, policies, and programs that shape
a community to best support the development of healthy relationships.
Each of us can start now, in our own lives, by strengthening our
connections and relationships. Our individual relationships are an
untapped resource—a source of healing hiding in plain sight. They
can help us live healthier, more productive, and more fulfilled lives.
Answer that phone call from a friend. Make time to share a meal. Listen
without the distraction of your phone. Perform an act of service. Express
yourself authentically. The keys to human connection are simple, but
extraordinarily powerful.
Vivek H. Murthy, M.D., M.B.A.
19th and 21st Surgeon General of the United States
Vice Admiral, United States Public Health Service
Each of us can start now, in our
own lives, by strengthening our
connections and relationships.
Loneliness and isolation represent profound threats to our health and
well-being. But we have the power to respond. By taking small steps
every day to strengthen our relationships, and by supporting community
efforts to rebuild social connection, we can rise to meet this moment
together. We can build lives and communities that are healthier and
happier. And we can ensure our country and the world are better poised
than ever to take on the challenges that lay ahead.
Our future depends on what we do today.

6Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
A Surgeon General’s Advisory is a public statement that calls the
American people’s attention to an urgent public health issue and provides
recommendations for how it should be addressed. Advisories are
reserved for significant public health challenges that require the nation’s
immediate awareness and action.
This advisory calls attention to the importance of social connection for
individual health as well as on community-wide metrics of health and
well-being, and conversely the significant consequences when social
connection is lacking. While social connection is often considered
an individual challenge, this advisory explores and explains the
cultural, community, and societal dynamics that drive connection and
disconnection. It also offers recommendations for increasing and
strengthening social connection through a whole-of-society approach.
The advisory presents a framework for a national strategy with specific
recommendations for the institutions that shape our day-to-day
lives: governments, health care systems and insurers, public health
departments, research institutions, philanthropy, schools, workplaces,
community-based organizations, technology companies, and the media.
This advisory draws upon decades of research from the scientific
disciplines of sociology, psychology, neuroscience, political science,
economics, and public health, among others. This document is not an
exhaustive review of the literature. Rather, the advisory was developed
through a substantial review of the available evidence, primarily found
via electronic searches of research articles published in English and
resources suggested by a wide range of subject matter experts, with
priority given to meta-analyses and systematic literature reviews. The
recommendations in the advisory draw upon the scientific literature and
previously published recommendations from the National Academies
of Sciences, Engineering and Medicine, the Centers for Disease Control
and Prevention, the American Heart Association, and the World
Health Organization.
The findings and recommendations in the advisory are also informed by
consultations with subject matter experts from academia, health care,
education, government, and other sectors of society, including more
than 50 identified experts who reviewed and provided individual detailed
feedback on an early draft that has informed this advisory.
For additional background and to read other Surgeon General’s
Advisories, visit SurgeonGeneral.gov
About the Advisory
LEARN MORE
Visit our website for more
information and resources
about social connection:
SurgeonGeneral.gov/Connection

7Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Belonging
A fundamental human need—the
feeling of deep connection with social
groups, physical places, and individual
and collective experiences.
5
Collective Efficacy
The willingness of community
members to act on behalf of
the common good of the group
or community
.
6
Empathy
The capability to understand and
feel the emotional states of others,
resulting in compassionate behavior.
7,8
Loneliness
A subjective distressing experience
that results from perceived
isolation or inadequate meaningful
connections, where inadequate refers
to the discrepancy or unmet need
between an individual’s preferred
and actual experience.
9,10
Norms of Reciprocity
A sense of reciprocal obligation that
is not only a transactional mutual
benefit but a generalized one; by
treating others well, we anticipate
that we will also be treated well.
11,12
Social Capital
The resources to which individuals
and groups have access through
their social connections.
13,14
The term
social capital is often used as an
umbrella for both social support
and social cohesion.
15
Social Cohesion
The sense of solidarity within
groups, marked by strong social
connections and high levels of social
participation, that generates trust,
norms of reciprocity, and a sense
of belonging.
13,15-18
Glossary
Social Connectedness
The degree to which any individual
or population might fall along the
continuum of achieving social
connection needs.
19
Social Connection
A continuum of the size and
diversity of one’s social network
and roles, the functions these
relationships serve, and their
positive or negative qualities.
10,19,20
Social Disconnection
Objective or subjective deficits in
social connection, including deficits
in relationships and roles, their
functions, and/or quality.
19
Social Infrastructure
The programs (such as volunteer
organizations, sports groups, religious
groups, and member associations),
policies (like public transportation,
housing, and education), and physical
elements of a community (such
as libraries, parks, green spaces,
and playgrounds) that support the
development of social connection.
Social Isolation
Objectively having few social
relationships, social roles, group
memberships, and infrequent
social interaction.
19,21
Social Negativity
The presence of harmful interactions
or relationships, rather than the
absence of desired social interactions
or relationships.
19,22
Social Networks
The individuals and groups a person is
connected to and the interconnections
among relationships. These “webs
of social connections” provide the
structure for various social connection
functions to potentially operate.
18,23
Social Norms
The unwritten rules that we follow
that serve as a social contract to
provide order and predictability
in society. The social groups we
belong to provide information and
expectations, and constraints on
what is acceptable and appropriate
behavior
.
24
Social norms reinforce
or discourage health-related and
risky behaviors (lifestyle factors,
vaccination, substance use, etc.).
25
Social Participation
A person’s involvement in activities
in the community or society that
provides interaction with others.
26,27
Social Support
The perceived or actual availability of
informational, tangible, and emotional
resources from others, commonly
one’s social network.
10,28
Solitude
A state of aloneness by choice that
does not involve feeling lonely.
Trust
An individual’s expectation of
positive intent and benevolence
from the actions of other people
and groups.
29-31

8Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Chapter 1
Overview
Introduction: Why Social Connection Matters
Our relationships and interactions with family, friends,
colleagues, and neighbors are just some of what create
social connection. Our connection with others and our
community is also informed by our neighborhoods, digital
environments, schools, and workplaces. Social connection—
the structure, function, and quality of our relationships
with others—is a critical and underappreciated contributor
to individual and population health, community safety,
resilience, and prosperity.
6,17,32-36
However, far too many
Americans lack social connection in one or more ways,
compromising these benefits and leading to poor health
and other negative outcomes.
People may lack social connection in a variety of ways, though it is often illustrated
in scientific research by measuring loneliness and social isolation. Social isolation
and loneliness are related, but they are not the same. Social isolation is objectively
having few social relationships, social roles, group memberships, and infrequent
social interaction.
19,21
On the other hand, loneliness is a subjective internal state.
It’s the distressing experience that results from perceived isolation or unmet need
between an individual’s preferred and actual experience.
9,10,19
The lack of social connection poses a significant risk for individual health and
longevity. Loneliness and social isolation increase the risk for premature death by
26% and 29% respectively.
37
More broadly, lacking social connection can increase
the risk for premature death as much as smoking up to 15 cigarettes a day.
4
In
addition, poor or insufficient social connection is associated with increased risk
of disease, including a 29% increased risk of heart disease and a 32% increased
risk of stroke.
38
Furthermore, it is associated with increased risk for anxiety,
depression,
39
and dementia.
40,41
Additionally, the lack of social connection may
increase susceptibility to viruses and respiratory illness.
42
KEY DATA
Lacking social connection
can increase the risk
for premature death as
much as smoking up to
15 cigarettes a day.

9Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
The lack of social connection can have significant economic costs to individuals,
communities, and society. Social isolation among older adults alone accounts
for an estimated $6.7 billion in excess Medicare spending annually, largely due
to increased hospital and nursing facility spending.
43
Moreover, beyond direct
health care spending, loneliness and isolation are associated with lower academic
achievement
44,45
and worse performance at work.
46-48
In the U.S., stress-related
absenteeism attributed to loneliness costs employers an estimated $154 billion
annually.
46
The impact of social connection not only affects individuals, but also
the communities they live in. Social connection is an important social determinant
of health, and more broadly, of community well-being, including (but not limited to)
population health, community resilience when natural hazards strike, community
safety, economic prosperity, and representative government.
13,15,17,34-36,49,50
What drives these profound health and well-being outcomes? Social connection
is a fundamental human need, as essential to survival as food, water, and shelter.
Throughout history, our ability to rely on one another has been crucial to survival.
Now, even in modern times, we human beings are biologically wired for social
connection. Our brains have adapted to expect proximity to others.
51,52
Our distant
ancestors relied on others to help them meet their basic needs. Living in isolation,
or outside the group, means having to fulfill the many difficult demands of survival
on one’s own. This requires far more effort and reduces one’s chances of survival.
52
Despite current advancements that now allow us to live without engaging with
others (e.g., food delivery, automation, remote entertainment), our biological need
to connect remains.
The health and societal impacts of social isolation and loneliness are a critical
public health concern in light of mounting evidence that millions of Americans lack
adequate social connection in one or more ways. A 2022 study found that when
people were asked how close they felt to others emotionally, only 39% of adults
in the U.S. said that they felt very connected to others.
53
An important indicator
of this declining social connection is an increase in the proportion of Americans
experiencing loneliness. Recent surveys have found that approximately half of
U.S. adults report experiencing loneliness, with some of the highest rates among
young adults.
1-3
These estimates and multiple other studies indicate that loneliness
and isolation are more widespread than many of the other major health issues of
our day, including smoking (12.5% of U.S. adults),
54
diabetes (14.7%),
55
and obesity
(41.9%),
56
and with comparable levels of risk to health and premature death.
Despite such high prevalence, less than 20% of individuals who often or always
feel lonely or isolated recognize it as a major problem.
57
CHAPTER 1: OVERVIEW
KEY DATA
Approximately half of
U.S. adults report
experiencing loneliness,
with some of the highest
rates among young adults.

10Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Together, this represents an urgent public health concern. Every level of increase
in social connection corresponds with a risk reduction across many health
conditions. Further, social connection can be a proactive approach to living a
fulfilled and happy life, enhancing life satisfaction, educational attainment,
and performance in the workplace, as well as contributing to more-connected
communities that are healthier, safer, and more prosperous.
Unsurprisingly, social connection is generally not something we can do alone and
not something that is accessible equitably. That is partially because we need others
to connect with, but also because our society —including our schools, workplaces,
neighborhoods, public policies, and digital environments—plays a role in either
facilitating or hindering social connection.
10,32
Moreover, it is critical to carefully
consider equity in any approach to addressing social connection, as access and
barriers to social opportunities are often not the same for everyone and often
reinforce longstanding and historical inequities.
This advisory calls attention to the critical role that social connection plays in
individual and societal health and well-being and offers a framework for how we
can all contribute to advancing social connection.
What is Social Connection?
Social connection can encompass the interactions, relationships, roles, and
sense of connection individuals, communities, or society may experience.
10, ,2019
An individual’s level of social connection is not simply determined by the number
of close relationships they have. There are many ways we can connect socially,
and many ways we can lack social connection. These generally fall under one of
three vital components of social connection: structure, function, and quality.
• Structure
The number of relationships, variety of relationships (e.g., co-worker, friend,
family, neighbor), and the frequency of interactions with others.
• Function
The degree to which others can be relied upon for various needs.
• Quality
The degree to which relationships and interactions with others are positive,
helpful, or satisfying (vs. negative, unhelpful, or unsatisfying).
These three vital components of social connection are each important for
health,
4,32
and may influence health in different ways.
20
CHAPTER 1: OVERVIEW

11Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
FIGURE 1: The Three Vital Components of Social Connection
CHAPTER 1: OVERVIEW
The three Vital Components of Social Connection
The extent to which an individual is socially c
onnected depends on multiple factors, including:
Structure the number of variety of relationships and frequency of interactions
Examples
Household size
Friend circle siz
e
Martial/partnership status
Function the degree to which relationships serv
e various needs
Examples
Emotional support
Mentorship
Support in a crisis
Quality The positi
ve and
negative aspects of
relationships and
interactions
Examples
Relationship satisfaction
Relationship strain
Social inclusion or exclusion
Source Hot-Lunstad J. Why Social Relationships Are Important for Physical Health: A Systems Approach to Understanding and odifying Risk and Protection.
Annu Rev Psychol.2018;69:437-438

12Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
It’s also critical to understand other defining features of social connection.
First, it is a continuum. Too often, indicators of social connection or social
disconnection are considered in dichotomous ways (e.g., someone is lonely
or they’re not), but the evidence points more to a gradient.
58,59
Everyone falls
somewhere on the continuum of social connection, with low social connection
generally associated with poorer outcomes and higher social connection with
better outcomes.
59
Second, social connection is dynamic. The amount and quality of social connection
in our lives is not static. Social connectedness changes over time and can be
improved or compromised for a myriad of reasons. Illness, moves, job transitions,
and countless other life events, as well as changes in one’s community and society,
can all impact social connectedness in one direction or another. Further, how
long we remain on one end of the continuum may matter. Transient feelings of
loneliness may be less problematic, or even adaptive, because the distressing
feeling motivates us to reconnect socially.
60
Similarly, temporary experiences of
solitude may help us manage social demands.
61
However, chronic loneliness (even
if someone is not isolated) and isolation (even if someone is not lonely) represent
a significant health concern.
21, ,63 62
Third, much like the absence of disease does not equate to good health, the
absence of social deficits (e.g., loneliness) does not necessarily equate to high
levels of social connection. Although some measures of social connection
represent the full continuum, others only focus on deficits, which do not capture
the degree to which social assets may contribute to resilience, or even enable
thriving.
58
Consider two examples: first, an individual who is part of a large,
highly-involved family, and second, an individual who has regular contact with
colleagues through work but has little time for personal relationships outside of
work. In each case, such an individual is not objectively isolated and may not feel
subjectively lonely. However, in both cases key measures of isolation and loneliness
may miss whether they are reaping the benefits of social connection in other ways,
such as feeling adequately supported or having high-quality, close relationships.
Current Trends: Is Social Connection Declining?
Across many measures, Americans appear to be becoming less socially connected
over time.
12,64
This is not a new problem—certain declines have been occurring
for decades. While precise estimates of the rates of social connection nationally
can be challenging because studies vary based on which indicator is measured,
when the same measure is used at multiple time points, we can identify trends.
CHAPTER 1: OVERVIEW

13Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Changes in key indicators, including individual social participation, demographics,
community involvement, and use of technology over time, suggest both overall
societal declines in social connection and that, currently, a significant portion of
Americans lack adequate social connection.
A fraying of the social fabric can also be seen more broadly in society. Trust
in each other and major institutions is at near historic lows.
65
Polls conducted
in 1972 showed that roughly 45% of Americans felt they could reliably trust
other Americans; however, that proportion shrank to roughly 30% in 2016.
66
This corresponds with levels of polarization being at near historic highs.
65,67
These phenomena combine to have widespread effects on society, including
many of the most pressing issues we face as a nation.
Trends in Social Networks and Social Participation
Social networks are getting smaller, and levels of social participation are declining
distinct from whether individuals report that they are lonely. For example, objective
measures of social exposure obtained from 2003-2020 find that social isolation,
measured by the average time spent alone, increased from 2003 (285-minutes/day,
142.5-hours/month) to 2019 (309-minutes/day, 154.5-hours/month) and continued
to increase in 2020 (333-minutes/day, 166.5-hours/month).
64
This represents an
increase of 24 hours per month spent alone. At the same time, social participation
across several types of relationships has steadily declined. For instance, the amount
of time respondents engaged with friends socially in-person decreased from 2003
(60-minutes/day, 30-hours/month) to 2020 (20-minutes/day, 10-hours/month).
64
This represents a decrease of 20 hours per month spent engaging with friends.
This decline is starkest for young people ages 15 to 24. For this age group, time
spent in-person with friends has reduced by nearly 70% over almost two decades,
from roughly 150 minutes per day in 2003 to 40 minutes per day in 2020.
64
The COVID-19 pandemic accelerated trends in declining social participation.
The number of close friendships has also declined over several decades.
Among people not reporting loneliness or social isolation, nearly 90% have three
or more confidants.
57
Yet, almost half of Americans (49%) in 2021 reported having
three or fewer close friends —only about a quarter (27%) reported the same in
1990.
68
Social connection continued to decline during the COVID-19 pandemic,
with one study finding a 16% decrease in network size from June 2019 to June 2020
among participants.
69
CHAPTER 1: OVERVIEW
KEY DATA
Polls conducted in 1972
showed that roughly 45%
of Americans felt they
could reliably trust other
Americans; however,
that proportion shrank
to roughly 30% in 2016.
14Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
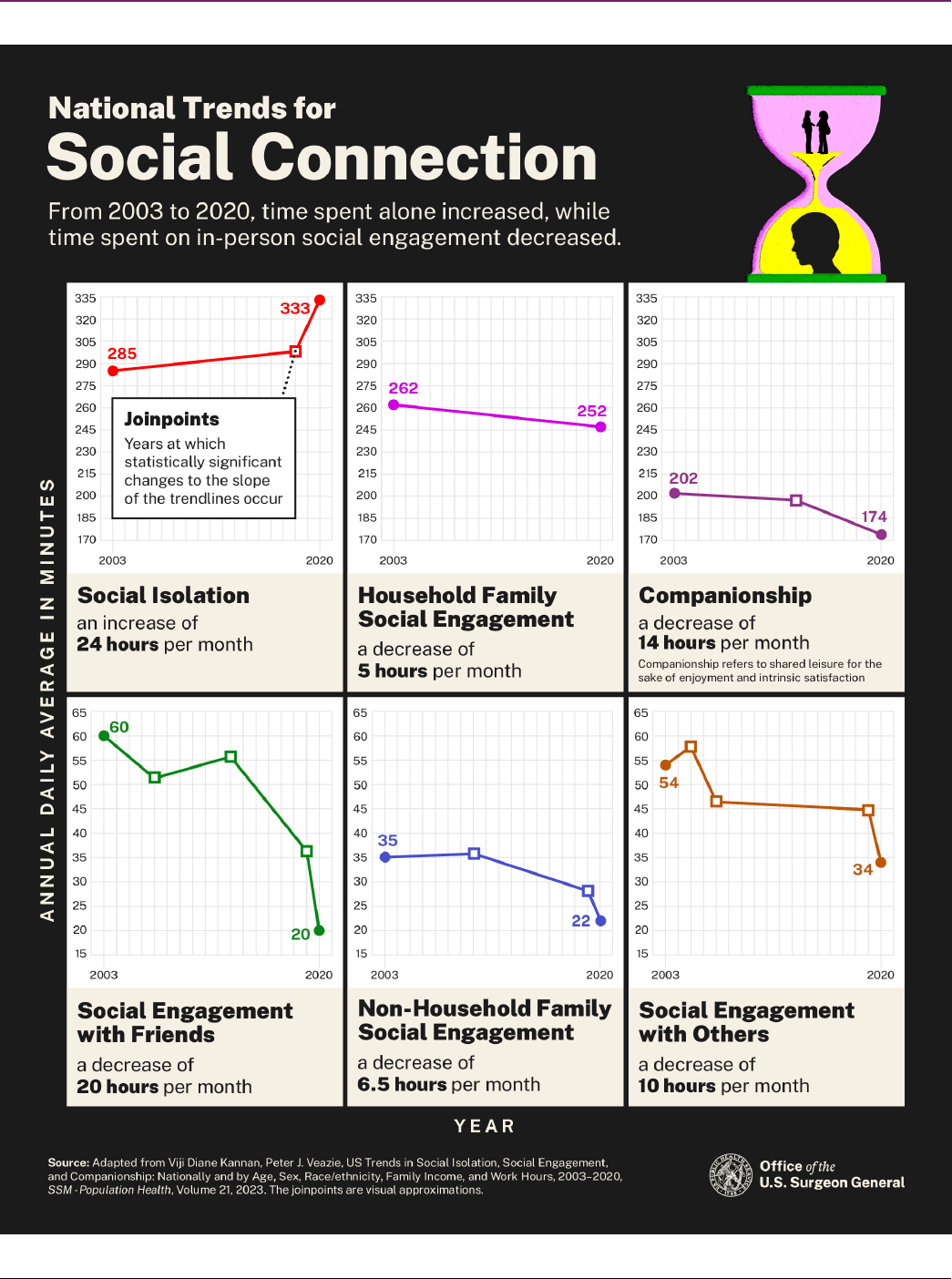
FIGURE 2: National Trends for Social Connection
CHAPTER 1: OVERVIEW
National Trends for Social Connection
From 2003 to 2020, time spent alone increased, while time spent on in-person social engagement decreased.
Social
Isolation
an
increase of
24 hours
per month
from 285
to 333
Household
Family
Social
Engagement
a decrease
of 5 hours
per month
from 262 to
2
5
2
Companio
nship a
decrease
of 14
hours per
month
companio
nship
refers to
shared
leisure for
the sake
of
enjoymen
t and
intrinsic
satisfactio
n from
202 to 174
Social
Engage
m
nte with
Friends
a decreas
e of 20
hours
pmeor nth
f6r0o to 20
Non-
household
Family
Social
Engagement
decrease of
6.5 hours
per month
from 35 to
22
Social
Engagement
with others
a decrease
of 10 hours
per
month
from
54 to 34
w
Source: Adapted from Viji Diane Kannan, Peter J. Veazie, US Trends in Social Isolation, Social Engagement, and Companionship: Nationally and by Age, Sex, Race/ethnicity, Family Income, and Work
Hours, 2003-2020, SSM-Population Health, Volume 21, 2023. The joinpoints are visual approximations. Office of the U.S. Surgeon General

15Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 1: OVERVIEW
Demographic Trends
Societal trends, including demographic changes such as age, marital/partnership
status, and household size, also provide clues to current trends. For example,
family size and marriage rates have been in steady decline for decades.
70
The percentage of Americans living alone has also increased decade-to-decade.
In 1960, single-person households accounted for only 13% of all U.S. households.
70
In 2022, that number more than doubled, to 29% of all households.
70
The reasons people choose to remain single or unmarried, have smaller families,
and live alone over time are complex and encompass many factors. Yet at the same
time, it is important to acknowledge the contribution these demographic changes
have on social disconnection because of the significant health impacts identified
in the scientific evidence. Moreover, awareness can help individuals consider these
impacts and cultivate ways to foster sufficient social connection outside of chosen
traditional means and structures.
The research in this section points to overall declines in some of the critical
structural elements of social connection (e.g., marital status, household size),
which helps to explain increases in reported loneliness and social isolation and
contributes to the overall crisis of connection we are experiencing. Finally, this
suggests we have fewer informal supports to draw upon in times of need—all while
the number of older individuals and those living with chronic conditions continues
to increase.
Awareness can help individuals
consider these impacts and cultivate
ways to foster sufficient social
connection outside of chosen
traditional means and structures.
KEY DATA
In 1960, single-person
households accounted
for only 13% of all U.S.
households. In 2022, that
number more than doubled,
to 29% of all households.

16Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Trends in Community Involvement
Although the concept of community has evolved over time, many traditional
indicators of community involvement, including with religious groups, clubs,
and labor unions, show declining trends in the United States since at least the
1970s.
12,71
In 2018, only 16% of Americans reported that they felt very attached
to their local community.
72
Membership in organizations that have been important pillars of community
connection have declined significantly in this time. Take faith organizations, for
example. Research produced by Gallup, Pew Research Center, and the National
Opinion Research Center’s General Social Survey demonstrates that since the
1970s, religious preference, affiliation, and participation among U.S. adults have
declined.
73-75
In 2020, only 47% of Americans said they belonged to a church,
synagogue, or mosque. This is down from 70% in 1999 and represents a dip
below 50% for the first time in the history of the survey question.
75
Religious
or faith-based groups can be a source for regular social contact, serve as a
community of support, provide meaning and purpose, create a sense of belonging
around shared values and beliefs, and are associated with reduced risk-taking
behaviors.
76-78
As a consequence of this decline in participation, individuals’ health
may be undermined in different ways.
16
What Leads Us to Be More or Less Socially Connected?
A wide variety of factors can influence an individual or community’s level of social
connection. One organizing tool that helps us better understand these factors is
the social-ecological model.
79,80
This model organizes the interrelated factors that
affect health on the individual level, in our relationships, in our communities, and
in society. Each of these levels—from the smallest to the broadest—contribute to
social connection and its associated risks and protection for health.
CHAPTER 1: OVERVIEW
16
KEY DAT
%
A
In 2018, only 16% of
Americans reported
that they felt very
attached to their
local community.

17Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
FIGURE 3: Factors That Can Shape Social Connection
CHAPTER 1: OVERVIEW
Factors That Can
Shape Social Connection
Individual
• Chronic disease
• Sensory and functional impairments
• Mental health
• Physical health
• Personality
• Race
• Gender
• Socioeconomic st
atus
• Life stage
Relationships
• Structure, function, and
quality
• Household size
• Characteristics and
behaviors of others
• Empathy
Community
• Outdoor space
• Housing
• Schools
• Workplace
• Local government
• Local business
• Community organiz
ations
• Health care
• Transportation
Society
• Norms and values
• Public policies
• Tech environment and use
• Civic engagement
• Democratic norms
• Historical inequities

18Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 1: OVERVIEW
Social connection is most often viewed as driven by the individual —one’s genetics,
health, socioeconomic status, race, gender, age, household living situation, and
personality, among other factors. These can influence motivation, ability, or access
to connect socially. As we’ve seen, the level of one’s connection is also dependent
on the structure, function, and quality of relationships. However, connectedness is
influenced by more than simply personal or interpersonal factors. It is also shaped
by the social infrastructure of the community (or communities) in which one is born,
grows up, learns, plays, works, and ages.
Social infrastructure includes the physical assets of a community (such as libraries
and parks), programs (such as volunteer organizations and member associations),
and local policies (such as public transportation and housing) that support the
development of social connection.
The social infrastructure of these communities is in turn influenced by broader
social policies, cultural norms, the technology environment, the political
environment, and macroeconomic factors. Moreover, individuals are simultaneously
influenced by societal-level conditions such as cooperation, discrimination,
inequality, and the collective social connectedness or disconnectedness of the
community.
23
All of these shape the availability of opportunities for social connection.
In sum, social connection is more than a personal issue. The structural and social
characteristics of the community produce the settings in which people build,
maintain, and grow their social networks.
36,81,82
Because many contributors to social
connection go beyond an individual’s control, in order to promote health, change
is needed across the full scope of the social-ecological model. While every factor
listed in Figure 3, as well as some not captured, can be important contributors to
social connection, it’s important to look across these levels. That gives us clues
to barriers to connection and the types of interventions which could successfully
increase social connection. This broader view can also help identify what places
groups at highest risk for social isolation and loneliness, as well as factors that
reinforce cycles of risk or resilience.
…in order to promote health, change
is needed across the full scope of the
social-ecological model.

19Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 1: OVERVIEW
Groups at Highest Risk for Social Disconnection
Anyone of any age or background can experience loneliness and isolation, but some
groups are at higher risk than others. Not all individuals or groups experience the
factors that facilitate or become barriers to social connection equally. Some people
or groups are exposed to greater barriers. It’s critical to examine and highlight the
disproportionate risk they face and to target interventions to address their needs.
Although risk may differ across indicators of social disconnection, currently,
studies find the highest prevalence for loneliness and isolation among people with
poor physical or mental health, disabilities, financial insecurity, those who live
alone, single parents, as well as younger and older populations.
1, ,
For example,
while the highest rates of social isolation are found among older adults,
8364
64
young
adults are almost twice as likely to report feeling lonely than those over 65.
1
The rate of loneliness among young adults has increased every year between 1976
and 2019.
84
In addition, lower-income adults are more likely to be lonely than those
with higher incomes. Sixty-three percent of adults who earn less than $50,000
per year are considered lonely, which is 10 percentage points higher than those
who earn more than $50,000 per year.
1
These data do not suggest that individual
or demographic factors inherently generate loneliness or isolation. Rather, the
data enable us to understand the different socioeconomic, political, and cultural
mechanisms that may indicate higher risk for certain groups and lead to loneliness
and isolation.
Additional at-risk groups may include individuals from ethnic and racial minority
groups, LGBTQ+ individuals, rural residents, victims of domestic violence, and
those who experience discrimination or marginalization. Further research is needed
to fully understand the disproportionate impacts of social disconnection.
Impacts of Technology on Social Connection
There is more and more evidence pointing to the importance of our environments
for health, and the same is true for digital environments and our social health.
A variety of technologies have quickly and dramatically changed how we live,
work, communicate, and socialize. These technologies include social media,
smartphones, virtual reality, remote work, artificial intelligence, and assistive
technologies, to name just a few.
These technologies are pervasive in our lives. Nearly all teens and adults under
65 (96-99%), and 75% of adults 65 and over, say that they use the internet.
85
Americans spend an average of six hours per day on digital media.
86
One-in-three
U.S. adults 18 and over report that they are online “almost constantly,”
87
and
KEY DATA
The rate of loneliness
among young adults has
increased every year
between 1976 and 2019.

20Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
the percentage of teens ages 13 to 17 years who say they are online “almost
constantly” has doubled since 2015.
88
When looking at social media specifically,
the percentage of U.S. adults 18 and over who reported using social media
increased from 5% in 2005 to roughly 80% in 2019.
89
Among teens ages 13 to 17
years, 95% report using social media as of 2022, with more than half reporting it
would be hard to give up social media.
88
Although tech adoption is relatively high
among all groups, Americans with disabilities,
90
adults with lower incomes,
91
and
Americans from rural areas
92
continue to experience a persistent, albeit shrinking,
digital divide. They are relatively less likely to own a computer, smartphone,
or tablet, or have broadband internet access.
90-92
Technology has evolved rapidly, and the evidence around its impact on our
relationships has been complex. Each type of technology, the way in which
it is used, and the characteristics of who is using it, needs to be considered
when determining how it may contribute to greater or reduced risk for social
disconnection. There are multiple meta-analyses
93-96
and reviews
97-105
examining
this topic that identify both benefits and harms.
Several examples of benefits include technology that can foster connection
by providing opportunities to stay in touch with friends and family, offering
other routes for social participation for those with disabilities, and creating
opportunities to find community, especially for those from marginalized
groups.
97,106-108
For example, online support groups allow individuals to share their
personal experiences and to seek, receive, and provide social support—including
information, advice, and emotional support.
95,104
Several examples of harms include technology that displaces in-person
engagement, monopolizes our attention, reduces the quality of our interactions,
and even diminishes our self-esteem.
97, ,110109
This can lead to greater loneliness,
fear of missing out, conflict, and reduced social connection. For example, frequent
phone use during face-to-face interactions between parents and children, and
between family and friends, increased distraction, reduced conversation quality,
and lowered self-reported enjoyment of time spent together in-person.
111-113
In a
U.S.-based study, participants who reported using social media for more than
two hours a day had about double the odds of reporting increased perceptions of
social isolation compared to those who used social media for less than 30 minutes
per day.
114
Additionally, targets of online harassment report feelings of increased
loneliness, isolation, and relationship problems, as well as lower self-esteem
and trust in others.
115
Evidence shows that even perpetrators of cyberbullying
experience weakened emotional bonds with social contacts and deficits in
perceived belongingness.
115
CHAPTER 1: OVERVIEW
KEY DATA
In a U.S.-based study,
participants who reported
using social media for
more than two hours a
day had about double
the odds of reporting
increased perceptions of
social isolation compared
to those who used social
media for less than
30 minutes per day.

21Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Understanding how technology can enhance or detract from social connection is
complicated by ever-changing social media algorithms, complex differences in
individual technology use, and balancing concerns over obtaining private user data.
Advancing research in this area is essential. With that said, the existing evidence
illustrates that we have reason to be concerned about the impact of some kinds of
technology use on our relationships, our degree of social connection, and our health.
CHAPTER 1: OVERVIEW
…the existing evidence illustrates
that we have reason to be concerned
about the impact of some kinds of
technology use on our relationships,
our degree of social connection,
and our health.
Risk and Resilience Can Be Reinforcing
The factors that facilitate, or become barriers to, social connection can also
reinforce either a virtuous or vicious cycle.
116
Economic status, health, and service
are just a few illustrative examples—better social connection can lead to better
health, whereas less social connection can lead to poorer health. However, each of
these can be reinforcing. Being in poorer health can become a barrier to engaging
socially, reducing social opportunities and support, and reinforcing a vicious
cycle of poorer health and less connection.
117-119
A similar kind of pattern could
occur among those struggling financially. For example, financial insecurity may
require someone to work multiple jobs, resulting in less leisure time and limiting
opportunities for social participation and connection—which, in turn, could provide
fewer resources and financial opportunities. While these cycles can be reinforcing,
they are not always negative. There is, for instance, a virtuous cycle between
social connection and volunteerism or service. Those who are more connected
to their communities are more likely to engage in service, and those who are
engaged in service are more likely to feel connected to their communities and the
individuals in it.
120
Interestingly, there is also evidence showing that the well-being
benefits associated with volunteering are even greater for those with higher social
connectedness than those with less.
121
Because these cycles can be reinforcing,
prioritizing social connection can not only disrupt vicious cycles but also reinforce
virtuous ones.

22Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
While social connection had been declining for
decades prior to the COVID-19 pandemic, the onset of
the pandemic, with its lockdowns and stay-at-home
orders, was a critical time during which the issue
of connection came to the forefront of public
consciousness, raising awareness about this critical
and ongoing public health concern.
Many of us felt lonely or isolated in a way we had
never experienced before. We postponed or canceled
meaningful life moments and celebrations like
birthdays, graduations, and marriages. Children’s
education shifted online—and they missed out on the
many benefits of interacting with their friends. Many
people lost jobs and homes. We were unable to visit our
children, siblings, parents, or grandparents. Many lost
loved ones. We experienced feelings of anxiety, stress,
fear, sadness, grief, anger, and pain through the loss of
these moments, rituals, celebrations, and relationships.
Although the COVID-19 pandemic was a collective
experience, it impacted certain populations differently.
Frontline workers had a different experience than
those who could work from home. Parents managing
their own work and their children’s online school had a
different experience than single young people unable
to interact in-person with friends. And those at greater
risk of severe COVID-19, including older individuals,
those living in nursing homes, and people with
underlying health conditions, faced unique challenges.
Emerging data suggests that people with close and
CALL OUT BOX
Lessons from the COVID-19 Pandemic
positive familial connections may have had a different
experience than those without. A recent national
survey showed that, by April 2021, 1 in 4 individuals
reported feeling less close to family members
compared to the beginning of the pandemic.
122
Yet, at the same time, about 1 in 5 said they felt closer
to family members,
122
perhaps indicating that the
pandemic exacerbated existing family dynamics of
connection or disconnection.
We also witnessed first responders, health care
workers, community members, neighbors, and
volunteers stepping up and offering their social
support to one another. Service can be a powerful
source of connection. From September 2020 to
September 2021, the majority (51%) of U.S. individuals
ages 16 and older reported informally helping
others.
123
This represents more than 120 million
U.S. individuals helping informally, in addition to an
estimated 60 million individuals formally volunteering
through an organization during the same period.
123
By engaging in service work, many were able to find
and create pockets of connection for themselves and
others during a public health crisis.
While profoundly disruptive in so many ways, the
COVID-19 pandemic offers an opportunity to reflect
more deeply on the state of social connection in our
lives and in society. As we emerge from this era,
rebuilding social connection and community offers
us a promising and hopeful way forward.
CHAPTER 1: OVERVIEW

23Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
How Social Connection
Impacts Individual
Health and Well-Being
Chapter 2
Extensive scientific findings from a variety of disciplines,
including epidemiology, neuroscience, medicine,
psychology, and sociology, converge on the same
conclusion: social connection is a significant predictor
of longevity and better physical, cognitive, and mental
health, while social isolation and loneliness are significant
predictors of premature death and poor health.
10, , ,1243220
In fact, the benefits of social connection extend beyond
health-related outcomes. They influence an individual’s
educational attainment, workplace satisfaction, economic
prosperity, and overall feelings of well-being and life
fulfillment. This chapter summarizes the rapidly growing
body of evidence on the relationship between various
indicators of social connection and these outcomes
for individuals.

24Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 2: INDIVIDUAL HEALTH
Individual Health Outcomes
Survival and Mortality
“Over four decades of research has produced
robust evidence that lacking social connection—
and in particular, scoring high on measures of
social isolation—is associated with a significantly
increased risk for early death from all causes.”
10
2020 Consensus Study Report,
National Academies of Sciences Engineering and Medicine
Evidence across scientific disciplines converges on the conclusion that socially
connected people live longer. Large population studies have documented that,
among initially healthy people tracked over time, those who are more socially
connected live longer, while those who experience social deficits, including
isolation, loneliness, and poor-quality relationships, are more likely to die earlier,
regardless of the cause of death.
37,125-128
Systematic research demonstrating
the link between social connection and mortality risk dates to one of the first
large-scale longitudinal epidemiological studies conducted in 1979.
129
This
research found that people who lacked social connection were more than twice
as likely than those with greater social connection to die within the follow-up
period, even after accounting for age, health status, socioeconomic status,
and health practices.
129
More recent estimates, based on synthesizing data across 148 studies, with an
average of 7.5 years of follow-up, suggest that social connection increases the
odds of survival by 50%.
128
Indeed, the effects of social connection, isolation, and
loneliness on mortality are comparable, and in some cases greater, than those of
many other risk factors (see Figure 4) including lifestyle factors (e.g., smoking,
alcohol consumption, physical inactivity), traditional clinical risks factors (e.g.,
high blood pressure, body mass index, cholesterol levels), environmental factors
(e.g., air pollution), and clinical interventions (e.g., flu vaccine, high blood pressure
medication, rehabilitation).
128,130
5
KEY D
0%
ATA
Data across 148 studies,
with an average of 7.5 years
of follow-up, suggest that
social connection increases
the odds of survival by 50%.

25Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
FIGURE 4: Lacking social connection is as dangerous as smoking up to 15 cigarettes a day.
Over the years, the number of studies, the rigor of their methods, and the size of
the samples have all increased substantially, providing stronger confidence in this
evidence. These replicate the finding that social connection decreases the risk of
premature death.
Taken together, this research establishes that the lack of social connection is
an independent risk factor for deaths from all causes, including deaths caused
by diseases.
131
CHAPTER 2: INDIVIDUAL HEALTH
Lacking social connection is as dangerous as smoking up to 15 cigarettes a day.
Lacking Social Connection has the highest
odds of Premature Mortality
Followed by Smoking up to 15 cigarettes
daily
Followed by Drinking 6 alcoholic drinks
daily
Followed by Physical inactivity
Followed by Obesity
Followed by Air pollution
Source: Holt-Lunstad J. Robles TF, Sbarra
DA. Advancing So
cial Connection as a Public
Health Priority in the United States.
American Psycholo
gy. 2017;72(6):517-530.
doi:10,1037/amp0000103. This graph is a
visual approximation.
Office of the U.S. Surgeon General

26Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 2: INDIVIDUAL HEALTH
Cardiovascular Disease
The evidence linking social connection to physical health is strongest in heart
disease and stroke outcomes.
10,58
Dozens of studies have found that social
isolation and loneliness significantly increase the risk of morbidities from these
conditions.
10, ,133132
Among this evidence, a synthesis of data across 16 independent
longitudinal studies shows poor social relationships (social isolation, poor social
support, loneliness) were associated with a 29% increase in the risk of heart
disease and a 32% increase in the risk of stroke.
38
Interestingly, these effects
can begin early in life and stretch over a lifetime. Research has also found that
childhood social isolation is associated with increased cardiovascular risk factors
such as obesity, high blood pressure, and blood glucose levels in adulthood.
133-135
Further, in a 2022 statement, the American Heart Association concluded that
“social isolation and loneliness are common, yet underrecognized, determinants
of cardiovascular health and brain health.”
133
Heart failure patients who reported high levels of loneliness had a 68% increased
risk of hospitalization, a 57% higher risk of emergency department visits, and
a 26% increased risk of outpatient visits, compared with patients reporting low
levels of loneliness.
136
Combining data from 13 studies on heart failure patients,
researchers found that poor social connection is associated with a 55% greater
risk of hospital readmission.
137
This was consistent across both objective and
perceived social isolation, including living alone, lack of social support, and poor
social network. Furthermore, evidence suggests that people who are less socially
connected, particularly those living alone, may be less likely to make it to the
hospital, increasing their risk of dying from a cardiac event.
138
Conversely, a heart
attack is less likely to be fatal for people living with others or who have more social
contacts, perhaps because of the immediate response and availability of help
during the event.
138
Hypertension
High blood pressure (hypertension) is one of the leading causes of cardiovascular
disease.
139
Several studies demonstrate that the more social support one has, the
greater the reduction in the possibility of developing high blood pressure, even
in populations who are at higher risk for the condition, such as Black Americans.
Greater social support in this group is associated with a 36% lower risk of high
blood pressure in the long-term.
140
Among older adults, the effect of social isolation
on hypertension risk is even greater than that of other major clinical risk factors
such as diabetes.
59
KEY DATA
A synthesis of data
across 16 independent
longitudinal studies shows
poor social relationships
(social isolation, poor
social support, loneliness)
were associated with a
29% increase in the risk
of heart disease and a
32% increase in the risk
of stroke.

27Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 2: INDIVIDUAL HEALTH
Since high blood pressure most often doesn’t have symptoms, it is possible for
people to be unaware of even severe underlying cases.
141
The disorder may remain
undiagnosed for years, which can elevate the risk for a wide range of physiological
complications.
141
However, among older adults, people with higher perceived
emotional support from family and friends, and with frequent exposure to
health-related information within their social networks, are significantly less
likely to have undiagnosed and uncontrolled hypertension.
142
The results of many research studies also reflect a strong correlation between
social connection and high blood pressure control. Regular participation in two or
more social or community-based groups
143
; emotional and informational support
from family, friends, professional contacts, community organizations, and peer
groups
144-146
; and frequent network interactions
142
may improve hypertension
management, including following treatment recommendations and long-term
lifestyle adjustments. Findings from the National Social Life, Health, and Aging
Project (NSHAP) suggest a “causal role of social connections in reducing
hypertension,” particularly in adults over the age of 50.
59
Diabetes
Evidence gathered over the last 25 years has demonstrated that social context
is important to the development and management of diabetes.
147
Population-based
studies show the impact of social connection on the development of type 2
diabetes and diabetic complications.
148,149
For example, social disconnection
(poor structural social support
150
and living alone
151
in men, low emotional support
in women,
152
and not having a current partner in women older than 70
153
) has been
linked to an increased risk for the development of type 2 diabetes. Furthermore,
living alone increased the risk of developing type 2 diabetes among women with
impaired glucose tolerance.
154
By contrast, social connection has been associated with better self-rated health
and disease management among individuals with diabetes.
155-157
The involvement
and support of family members has also been repeatedly shown to improve disease
management and the health of people with type 1 diabetes and type 2 diabetes.
147
Whereas, smaller social network size has been associated with newly diagnosed
type 2 diabetes and complications from diabetes.
148,149
These associations between
social connection and broader diabetic outcomes including diagnosed pre-diabetes
and type 2 diabetes, macrovascular complications (e.g., heart attack, stroke) and
microvascular complications (e.g., diabetic retinopathy, impaired sensitivity in
the feet, and signs of kidney disease) were independent of blood sugar (glucose)
control, quality of life, and other cardiac risk factors.
148,149
KEY DATA
The involvement and
support of family members
has been repeatedly
shown to improve disease
management and the
health of people with
type 1 diabetes and
type 2 diabetes.

28Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
What explains this phenomenon? Diabetic outcomes may be better among people
who are more socially connected due to better diabetic management behaviors
and patient self-care such as medication adherence, physical activity, diet, and
foot care. For example, in a meta-analysis of 28 studies, social support from
family and friends was significantly associated with better self-care, particularly
blood sugar monitoring.
158
Finally, evidence from the National Health and Nutrition
Examination Survey found that among older adults with diabetes, those with
a large social support network size (at least six close friends) had a reduced risk
of all-cause mortality.
159
Infectious Diseases
People who are less socially connected may have increased susceptibility and
weaker immune responses when they are exposed to infectious diseases. In a
series of studies examining factors that contribute to illness after exposure to
viruses like the common cold and flu, loneliness and poor social support were
found to significantly contribute to the development and severity of the illnesses.
42,160
In one study where participants were exposed to a common cold virus, individuals
with social ties to six or more diverse social roles (e.g., parent, spouse, friend,
family, co-worker, group membership) had a four-fold lower risk of developing a
cold when compared to people who had ties to fewer (1-3) diverse social roles.
161
These effects cannot be explained by previous exposure, since those who are
more socially connected have stronger immune responses independent of baseline
antibody count—suggesting stronger immune responses even when exposed to
new viruses.
42
A study conducted on immune responses to the COVID-19 vaccine
found that a lack of social connection with neighbors and resultant loneliness was
associated with weaker antibody responses to the vaccine.
162
Cognitive Function
Substantial evidence also links social isolation and loneliness with accelerated
cognitive decline and an increased risk of dementia in older adults,
10,41
including
Alzheimer’s disease.
163
Chronic loneliness and social isolation can increase the
risk of developing dementia by approximately 50% in older adults, even after
controlling for demographics and health status.
41
A study that followed older adults
over 12 years found that cognitive abilities declined 20% faster among those who
reported loneliness.
164
CHAPTER 2: INDIVIDUAL HEALTH
5
KEY D
0%
ATA
Chronic loneliness and
social isolation can
increase the risk of
developing dementia
by approximately 50%
in older adults.

29Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
When taken together, this evidence consistently shows that wider social networks
and more frequent social engagements with friends and family are associated with
better cognitive function and may protect against the risk of dementia.
40,165
This suggests that investments in social connection may be an important public
health response to cognitive decline.
Depression and Anxiety
Depression and anxiety are often characterized by social withdrawal, which
increases the risk for both social isolation and loneliness; however, social isolation
and loneliness also predict increased risk for developing depression and anxiety
and can worsen these conditions over time. A systematic review of multiple
longitudinal studies found that the odds of developing depression in adults is more
than double among people who report feeling lonely often, compared to those who
rarely or never feel lonely.
39
Furthermore, in older adults, both social isolation and
loneliness have been shown to independently increase the likelihood of depression
or anxiety.
166
These findings are also consistent among younger people. A review
of 63 studies concluded that loneliness and social isolation among children and
adolescents increase the risk of depression and anxiety, and that this risk remained
high even up to nine years later.
167
Importantly, social connection also seems to protect against depression even
in people with a higher probability of developing the condition. For example,
frequently confiding in others is associated with up to 15% reduced odds of
developing depression among people who are already at higher risk due to their
history of traumatic or otherwise adverse life experiences.
168
Suicidality and Self-Harm
CHAPTER 2: INDIVIDUAL HEALTH
KEY DATA
Loneliness and social
isolation among children
and adolescents
increase the risk of
depression and anxiety.
“Social isolation is arguably the strongest and most
reliable predictor of suicidal ideation, attempts, and
lethal suicidal behavior among samples varying in
age, nationality, and clinical severity.”
169
2010 Study, “The Interpersonal Theory of Suicide”
While many factors may contribute to suicide, more than a century of research has
demonstrated significant links between a lack of social connection and death by
suicide. This research suggests that social connection may protect against suicide
as a cause of death, especially for men.

30Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 2: INDIVIDUAL HEALTH
One study found that among men, deaths due to suicide are associated with
loneliness and more strongly with indicators of objective isolation such as living
alone.
170
In this study of over 500,000 middle-aged adults, the probability of
dying by suicide more than doubled among men who lived alone. The same study
showed that for women loneliness was significantly associated with hospitalization
for self-harm.
170
Further, when examining suicidality among nursing home and
other long-term care facility residents,
171
cancer patients,
172
older adults,
173
and
adolescents,
174
systematic reviews of studies on loneliness, social isolation, and low
social support were associated with suicidal ideation. These links may result from
a low sense of belonging and perceiving oneself as a burden to others.
169
Loneliness and low social support are also associated with increased risk of
self-harm. In a review of 40 studies of more than 60,000 older adults, an increase
in loneliness was reported to be among the primary motivations for self-harm.
175
Given the totality of the evidence, social connection may be one of the strongest
protective factors against self-harm and suicide among people with and without
serious underlying mental health challenges.
Social Connection Influences Health
Through Multiple Pathways
While the effects of social connection on health are clear, research also helps
explain how our level of social connection ultimately results in better or worse
health. A key part of the explanation involves understanding how social connection
influences behavioral, biological, and psychological processes, which in turn
influence health outcomes. A large body of evidence has identified several
plausible pathways (see Figure 5).
59,176-180

31Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
FIGURE 5: How Does Social Connection Influence Health?
CHAPTER 2: INDIVIDUAL HEALTH
How Does Social Connection Influence Health?
Social connection influences health through three principal pathways: biology, psychology, and behavior.
Components
Social Connection
Processes
Biology Stress Hormones, Inflammation, Gene Expression
Psychology Meaning/Purpose, Stress, Safety, Resilience,
Hopefulness
Behaviors Physical Activity, Nutrition,
Sleep, Smoking Treatment
Outcomes
Health Outcomes such as heart disease,
stroke, and diabetes can lead to an
individual's morbidity and premature
mortality.
Source: Holt-Lundtad J. The Major Health Implications of Social Connection. Current Directions in Psychological Science. 2021;30(3):251-259. Office of the U.S. Surgeon General

32Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 2: INDIVIDUAL HEALTH
Social Connection Influences Biological Processes
The role of social connection on biology emerges early in life and continues
across the life course, contributing to risk and protection from disease.
59
Several
reviews document that social connection can influence health through specific
biological pathways, including cardiovascular and neuroendocrine dysregulation,
181
immunity,
42,177,182-184
and gut-microbiome interactions.
185,186
Because regulation of
these systems is critical for good health, the documented influence between social
connection and these biological pathways likely explains the impact on the risk of
the development of disease.
Biological systems often do not operate independently. This means that increases
in blood pressure, circulating stress hormones, and inflammation may occur
simultaneously, potentially compounding risk across several biological systems.
187
One biological pathway of great interest is inflammation, given that it has been
implicated as a factor in many chronic illnesses.
188
Evidence shows that being
objectively isolated, or even the perception of isolation, can increase inflammation
to the same degree as physical inactivity.
59
Similarly, lower social support is
associated with higher inflammation.
189,190
Chronic inflammation throughout the
body has been linked to various chronic illnesses across the lifespan, such as
cardiovascular disease, cancer, diabetes, depression, and Alzheimer’s disease,
as well as a variety of mental, cognitive, and physical health outcomes
188,191
that
increase the risk of premature mortality. Thus, inflammation may be a common
pathway that explains the many diverse health outcomes associated with isolation
and loneliness.
The protective, or positive, effects of social connection may operate on biological
systems in a similar way, meaning that social connection may reduce the risk of
disease by reducing biological system dysregulation. For example, increased levels
of social connection can improve various biomarkers of cardiovascular functioning,
including blood pressure,
192
cardiovascular reactivity,
193
and oxidative stress.
194
In addition, social support and social bonding are associated with better regulation
of the neuroendocrine system, including the role of oxytocin in both early life and
adult attachment.
181,195-197

33Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Social Connection Influences Psychological Processes
Social connection can also influence health through psychological processes,
such as the sense of meaning and purpose. Adults across the globe rate their social
relationships, particularly with family and close friends, as the most important
source of meaning, purpose, and motivation in their lives.
198
A sense of meaning
positively contributes to health because it motivates greater self-regulation in
pursuing goals—including health goals.
180
Furthermore, evidence suggests that
individuals with higher purpose and perceived emotional and practical support
from their social networks are more likely to engage in health-promoting behaviors,
such as the use of preventive health care services.
199,200
Other psychological processes, including the perception of stress, may also have
implications for health because they can influence our biology and behavior.
For example, higher social connection provides increased opportunities for and
access to support, thus reducing the likelihood of perceiving challenging situations
as stressful and helping us cope with stressful situations to minimize their
impact.
28,201
Conversely, being isolated or in poor quality relationships can increase
the likelihood that one perceives potential challenges as stressful. This stress may
be heightened because the individual has less support and fewer resources to draw
upon to cope with the situation.
28,201
Though certain forms of manageable, short-term challenges can boost
performance and motivation in day-to-day life, chronic stress and cumulative
biologic burden can contribute to worsened health outcomes. For example,
stress can contribute to poorer health-related behaviors, cause disruptions in
brain development, and increase the risk for mental health conditions and other
health problems such as obesity, heart disease, and diabetes.
202-205
Additionally,
while loneliness, poor-quality relationships, and social negativity can aggravate
stress responses and influence long-term health outcomes,
206
being more socially
connected can buffer against maladaptive stress responses and the negative
health effects of stress.
28,201
CHAPTER 2: INDIVIDUAL HEALTH
A sense of meaning positively
contributes to health because it
motivates greater self-regulation in
pursuing goals—including health goals.
KEY DATA
Adults across the
globe rate their social
relationships, particularly
with family and close
friends, as the most
important source of
meaning, purpose, and
motivation in their lives.

34Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 2: INDIVIDUAL HEALTH
Social Connection Influences Behaviors
Social connection is also significantly associated with a number of health-related
behaviors, including lifestyle behaviors (e.g., diet, exercise, sleep),
207-210
and treatment adherence (e.g., taking medication as directed, engaging in
recommended prevention measures)
144, , ,212211199
which ultimately influence our
health and longevity. Social influence can be direct—loved ones encouraging one
to get more sleep or reminding one to take their medication—or subtle, through
social norms that communicate approval or disapproval of certain behaviors
(like vaccination, smoking, exercise). In fact, evidence shows people are far more
likely to be physically active if their peers and friends also exercise,
213,214
and they
are more likely to stop smoking themselves if their social contacts do so as well.
215
However, they are also less likely to stop smoking if they are in close connection to
others who smoke, or even at risk for relapse if they had successfully quit smoking
previously.
216,217
Thus, it is clear that it is not just the presence of social connection
and social support but the nature of the behaviors and norms in one’s social
network that influence health-related behaviors.
Individual Educational and Economic Benefits
The benefits of social connection extend beyond the well-being of individuals’
health to quality of life, education, employment, and economic outcomes. Just as
with health, those who lack sufficient social connection, whether because they are
isolated, lonely, or in poor-quality relationships, seem to be at higher risk for poorer
outcomes in these aspects of life as well.
Educational Benefits
Research shows that children and adolescents who enjoy positive relationships
with their peers, parents, and teachers experience improved academic outcomes.
For example, a review of youth mentoring programs found a positive association
between mentoring programs intended to promote positive youth outcomes and
improved school attendance, grades, and academic achievement test scores.
218
Further, school and family connectedness during adolescent years may predict
subsequent positive outcomes in early adulthood, including a higher likelihood of
graduating college and attaining a 4-year college degree.
219
In contrast, the lack of quality social connections inhibits student progression even
in higher education settings. For example, among medical students, feeling socially
isolated is associated with dropping out.
45
The lack of social connection is cited as
a prime reason for leaving a program.

35Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 2: INDIVIDUAL HEALTH
Economic Benefits
Supportive and inclusive relationships at work are associated with employee job
satisfaction, creativity, competence, and better job performance.
220-224
Quality
social support, social integration, and regular communication among co-workers
of all levels are key in preventing chronic work stress and workplace burnout.
48,
225
These resources may even be linked to shorter recovery times and less missed
work after work-related injuries or illnesses.
225,226
Workplace connectedness is
also associated with enhanced individual innovation, engagement, and quality
of work, all of which can influence career advancements, income, and overall
economic stability.
220,223
Social connection outside the workplace also plays an important role in an
individual’s economic situation. Diverse social networks that facilitate interaction
and relationship-building among people of differing socioeconomic status (SES)
may provide opportunities for individuals from lower SES backgrounds to gain
stronger footing in the labor market and obtain higher-paying jobs.
227,228
Such
bridging, cross-class ties are among the most important predictors of upward
economic mobility.
Additionally, activities that better connect individuals to one another, including
immersion in local community-based activities or volunteering, can also equip
individuals with desirable skills that make them more employable, and significantly
increase the likelihood of unemployed individuals becoming employed.
229-231

36Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
How Social Connection
Impacts Communities
Chapter 3
Decades of research across disciplines such as political
science, economics, sociology, behavioral science, and
public health, among others, have examined the relationship
between group social connection and population health
and well-being.
13, , , , , 504934-361715
Though variation exists across
studies and methodologies, the cumulative evidence
generally points to the same conclusion: higher levels of
social connectedness suggest better community outcomes,
ranging from population health to community safety,
resilience, prosperity, and representative government;
while lower levels of social connectedness suggest worse
outcomes in each of these areas. These studies establish
that social connection is vital not only to our individual
physical, mental, and emotional health, but also to the
health and well-being of our communities.
This chapter explores what it means to be a socially connected community and
examines the evidence that more connected communities benefit from higher
levels of well-being. The chapter also addresses the potential harms of negative
social connection for community and societal well-being.

37Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 3: COMMUNITY HEALTH
Socially Connected Communities
The scientific literature on social connection has defined “community” in many
ways.
232,233
Broadly, the term refers to a group of people with a characteristic in
common. For the purpose of this advisory, however, the terms “community” and
“communities” refer to a shared geographic location—neighborhoods, towns, cities.
This chapter summarizes research that pertains to in-person social connection and
the benefits that exist within place-based communities.
This does not diminish other types of communities (including those online) that can
also provide support and other important elements of social connection. However,
in-depth review of these types of communities is beyond the scope of this advisory
and requires additional research.
Social capital is a key concept that researchers have identified as an important
characteristic for understanding the social connectedness of communities.
The definition and measurement of social capital varies by discipline, but broadly,
social capital may be understood as “the resources to which individuals and groups
have access through their social networks.”
13,14
The term social capital is often used
as an umbrella for both social support and social cohesion.
15
Social support refers to the perceived or actual availability of emotional,
informational, or tangible resources from other individuals in one’s social network.
10,28
Social cohesion refers to the sense of solidarity within groups, marked by strong
social connections and high levels of social participation, that generates trust,
norms of reciprocity, and a sense of belonging.
13, , ,181715
Trust is a critical component of socially connected communities and a subjective
indicator frequently used to measure social capital.
15
Again, the scientific
literature defines trust in many ways, but, broadly, it refers to an individual’s
expectation of positive intent and benevolence from the actions of others.
29-31
Trust is an attitude that informs behavior towards unknown people (generalized
trust), towards a known individual or group (particularized trust), or towards
organizations and government (institutional trust).
29,234
It underlies communication
and cooperation, both elements of social cohesion and social support. Higher levels
of trust have been linked to improved population health, economic prosperity, and
social functioning.
15,235
The social infrastructure of a community shapes its social capital. This refers to
the programs (such as volunteer organizations, sports groups, religious groups, and
member associations), policies (like public transportation, housing, and education),
and physical elements of a community (such as libraries, parks, green spaces, and
playgrounds) that facilitate bringing people together. Social infrastructure may
help a community by providing opportunities to foster social connections among

38Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
residents, local leaders, and community-serving organizations. As social networks
grow in size, diversity, and strength, this produces greater levels of social support
and social cohesion and builds social capital for a community.
Because belonging to a group is generally adaptive and improves survival, people
have a natural tendency to build and maintain relationships with those who are
most like themselves (e.g., those with similar educational backgrounds, incomes,
professions, or family status).
236
This type of social connection, defined as bonding
social capital, is important and can provide the support and resources needed not
only to prevent or reduce loneliness and social isolation but also to contribute to
fulfillment and well-being.
237,238
Research suggests that diversifying social relationships to include connections
with people who are outside of your group (bridging social capital), as well
as connections between people of differing power status in the community
(linking social capital) are also associated with improved community health and
well-being.
13,237-239
Examples of these types of relationships include cultivating
intergenerational friendships (bridging) or developing programs like a mentorship
exchange between youth and local employers (linking).
Larger and more diverse social networks, with a mixture of types of relationships, can
provide access to more varied types of social support and generate greater levels
of social capital. Furthermore, interacting with people from diverse backgrounds
can help to stimulate creative thinking and encourage the consideration of different
perspectives, leading to better problem-solving and decision-making. Finally,
social interactions with neighbors and other community members —like small
gestures such as smiling at a passerby or brief conversations at the bank, post
office, grocery store, or local coffee shop—can foster a sense of interpersonal trust
and create and maintain norms of reciprocity.
240
12,241
This can also increase empathy,
one of the best documented sources of altruism, by enhancing understanding with
one another, supporting the development of shared identities and affiliations, and
facilitating cooperation and beneficial interactions across individuals and groups.
7,8
This helps to generate more social capital for the broader community.
These community interactions can be associated with a positive reinforcing cycle.
As this chapter illustrates, individuals who immerse themselves in community-based
activities are more likely to experience stronger feelings of social belonging
and develop trusting relationships with fellow community members. This can
lead people to more readily contribute their time and resources back to their
communities. When community-based participation becomes the norm, social
networks grow and produce high levels of trust among themselves, which
facilitates the efficient exchange of information and sharing of resources within
a community.
CHAPTER 3: COMMUNITY HEALTH

39Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 3: COMMUNITY HEALTH
The Benefits of More Connected Communities
Population Health
Communities with higher levels of social connection typically enjoy significantly
better health outcomes than communities that have lower levels.
16, , 242-24417
Studies
find that community-level social capital is positively associated with a reduced
burden of disease and risk for all-cause mortality.
17, ,245-247243
A meta-analysis of
several studies looking at the cumulative effects across multiple indicators of
social capital on all-cause mortality and general health found that on average,
a one-unit increase in social capital increases the likelihood of survival by 17%
and of self-reporting good health by 29%.
243
In a separate study using data from
39 states, the authors found a dose-response relationship between the extent of
social capital within a community and age-adjusted mortality.
248
A 10% increase
(one standard deviation) in the proportion of residents in each state who felt
that other people could be trusted was associated with an 8% decline in overall
mortality.
248
Another study found that those with very strong perceptions of
community belonging—an indicator of social cohesion—reported very good or
excellent health at a rate 2.6 times higher than those with very low perceptions
of belongingness.
245
This was true even after adjusting for demographic variables,
health and health behaviors, and the built environment. Finally, communities
with higher levels of social capital are also more likely to see decreased hospital
readmission rates.
249
The positive effects of social capital on health are not only evident when added
up across individuals. Synergistic effects among various aspects of social capital
also exist and impact community-wide health outcomes. Connected individuals
who leverage available social capital resources to improve their health-related
behaviors or collectively reform their community culture can generate downstream
improvements in overall population-level health.
For example, personal biases and fears about highly stigmatized diseases such
as HIV create barriers to health care and social inclusion for individuals living
with HIV.
250,251
A review of multiple studies shows that high levels of social capital
in high-risk populations can buffer against those harmful social barriers and
significantly increase the likelihood of HIV prevention behaviors.
250, ,253252
In turn, members of highly connected communities are more likely to participate
in health-protective efforts and seek care when needed, thereby decreasing the
disease burden and risk of disease transmission among the whole population.
Similarly, more connected communities have higher utilization of immunization
services, and are more likely to adopt recommended health-protective behaviors—
all of which benefit the broader community.
254-258
KEY DATA
On average, a one-unit
increase in social capital
increases the likelihood
of survival by 17% and
of self-reporting good
health by 29%.

40Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Evidence also shows that stronger social bonds and social capital in communities
increase the likelihood that local community groups and health care institutions
will build population health-focused partnerships.
259
These partnerships rely on
the existing mutual trust and reciprocity within community settings to increase
engagement opportunities within the population and improve access to health care
in low-resource populations.
259,260
On the other hand, several reports have found that lower community social
connection is linked to poorer health outcomes. This was made clear when
examining the spread of the COVID-19 virus.
261-264
One study in the United States
compared changes in the county-level spread of COVID-19 against several
measures of social capital.
265
These included family structure and involvement,
trust in community institutions, popularity of volunteerism, levels of participation in
political discussions and voting efforts, and cohesion among community members.
After controlling for potential alternative explanatory factors, the researchers
found that lower levels of social capital were associated with a higher number of
cases and deaths from COVID-19 infection.
265
Further, counties with strong social
ties experienced fewer deaths during the COVID-19 pandemic.
263,265
Relatedly, an
international study of COVID-19 infection and fatality rates across 177 countries
also observed a statistically significant association between greater interpersonal
and government trust and lower infection rates.
266
Natural Hazard Preparation and Resilience
A community’s resilience to natural hazard events such as earthquakes, tsunamis,
hurricanes, large-scale flooding, and fires depends upon the collective ability of
individuals, households, and institutions to prepare for anticipated events, adapt to
and withstand changing conditions, and recover rapidly following disruption.
267,268
Studies show that neighbors are often the first to respond in disaster situations,
even before trained emergency professionals, because they are physically
nearby.
34
Growing evidence suggests that in neighborhoods and communities
where people know one another and are connected to community institutions (like
service organizations, religious groups, or community-based organizations) people
prepare for, respond to, and recover more quickly from natural hazards than those
with lower levels of social connection.
232,269
In such connected communities, it is more likely that people will share their
knowledge and informal resources with neighbors, prepare for natural hazards,
comply with emergency procedures including evacuation, and engage in
coordination of emergency response efforts after natural hazard events.
35,270
CHAPTER 3: COMMUNITY HEALTH

41Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Further, high levels of social connection reduce the exodus of people immediately
following a natural hazard, preserve valuable social capital like social support
and interpersonal trust, enable neighbors to provide aid to one another, and allow
communities to overcome collective action problems such as coordinating recovery
and rebuilding.
35
Despite these benefits of connection within and for neighborhood
communities, only 3 in 10 Americans report knowing all or most of their neighbors.
72
Community Safety
Not only do higher levels of social connection within a community correspond to
better health and disaster outcomes, but they are also associated with lower levels
of community violence.
271-274
One recent study on community violence showed that
a one standard deviation increase in social connectedness was associated with
a 21% reduction in murders and a 20% reduction in motor vehicle thefts.
271
The Project on Human Development in Chicago Neighborhoods longitudinal study
that began in the late 1990s found that neighborhoods with higher perceptions
of social cohesion and where residents felt a “willingness to act” on behalf of
community members (collective efficacy) were more likely to have reduced levels
of crime and residents were more likely to feel safer.
6
Many subsequent analyses
have confirmed the association between social connection, greater perceived
collective efficacy, and community safety. Recent studies have found that greater
perceived collective efficacy,
49, ,276275
trust,
277
and social norms on violence as
unacceptable behavior can be protective factors against community violence.
278,279
Fostering social connection is not a singular solution to community violence;
however, it does play an instrumental role in prevention and response.
Economic Prosperity
Economic prosperity, including economic development, employment, the sharing
of economic opportunities or information, and overall economic connectedness,
is a key measure of the value that exists within a given society. Evidence illustrates
that connected communities generally experience higher levels of economic
prosperity. For example, an analysis of economic factors across the U.S. found
that communities with higher social capital levels experienced greater resilience
against unemployment between 2006 and 2010 and were able to weather the
recession more successfully.
280
In addition, a three-year study of 26 cities in the
U.S. found that those with the highest levels of resident attachment experienced
the greatest growth in GDP during the study period.
281
CHAPTER 3: COMMUNITY HEALTH
KEY DATA
A three-year study of 26
cities in the U.S. found
that those with the
highest levels of resident
attachment experienced
the greatest growth in GDP
during the study period.
KEY DATA
One recent study on
community violence
showed that a one standard
deviation increase in
social connectedness was
associated with a 21%
reduction in murders and
a 20% reduction in motor
vehicle thefts.

42Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Further, members of these connected communities are more likely to recommend
job and educational opportunities to one another, collaborate on ideas for
innovation, build partnerships for local businesses, and directly advance economic
progress in their communities.
280,282
In addition, longitudinal evidence shows that
civic engagement, another form of community participation, in adolescence and
early adulthood positively predicts educational attainment and income potential
in adulthood.
283
In this way, local community participation may also influence
socioeconomic mobility of individuals across their lifespan and also reduce
large-scale socioeconomic disparities.
CHAPTER 3: COMMUNITY HEALTH
In contrast to the clear benefits of community connectedness, the consequences
of disconnection on community prosperity can be detrimental. Long-standing
systemic disinvestment, inequitable zoning laws, underdeveloped transportation
systems, and residential segregation can perpetuate chronic poverty and isolate
entire neighborhoods or towns from more prosperous local economies.
36
On the
other hand, cross-class exposure could have positive impacts on economic mobility
across generations.
227
For example, if children of low socioeconomic backgrounds
had the share of high socioeconomic friends comparable to that of the average
child with a high socioeconomic background, these children would increase
their incomes in adulthood by an average of 20%.
227
Pro-connection policies and
practices can promote economic prosperity in communities harmed by structural
barriers and eliminate such obstacles toward prosperity.
Civic Engagement and Representative Government
Higher levels of social connection are associated with increased levels of civic
engagement (defined as “actions to address issues of public concern”) and
more representative government.
15, ,28450
Emerging evidence has shown that civic
engagement helps to develop “empathy, problem solving, [and] cooperation”
among community members.
285
One study showed that higher levels of family and
community connection during adolescence predicted civic engagement outcomes
in young adulthood including a greater likelihood of voting and involvement in
social action and conversation groups.
286
Further examples of civic engagement
include registering to vote and voting, participating in advocacy groups or clubs,
Local community participation may influence
socioeconomic mobility of individuals across
their lifespan and also reduce large-scale
socioeconomic disparities.

43Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 3: COMMUNITY HEALTH
and connecting to information and current events. In addition, studies show
that group membership and social networks strongly influence the decision
to participate in the political process.
287
Moreover, in a positive cycle, research
suggests that greater civic engagement can lead to policies and programs that
better reflect the will of a community’s residents, which in turn can promote
continued and increased civic engagement.
15, , ,289288284
The Potential Negative Side of Social Connection
Our fundamental human need for belonging is so strong that we may seek it out
even in ways that may be unhealthy to ourselves or to our broader community. This
can include participation in gangs and joining extremist or other harmful groups.
Our natural tendency to associate with those most like us can be manipulated, with
potentially negative consequences for individual and community well-being. When
there are scarce resources, this can also lead to competition among various groups,
leading to an “us” versus “them” mentality.
We tend to view our own group as more favorable and deserving than members of
other groups.
290
This can result in distrust and rejection of outsiders.
291
In addition,
among highly cohesive groups, there are also strong pressures to conform to the
group norms
292
—often with high costs like rejection or ostracization if one doesn’t
comply. While high cohesion and conformity to group norms can be healthy and
productive in many cases, among some groups, these social pressures may justify,
rationalize, or encourage unhealthy, unsafe, or unfair behaviors such as binge
drinking, violence, and discrimination.
274,292

44Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Societal Polarization
One consequence of the natural tendency for people to build and maintain
relationships with those who are like themselves is the risk for exacerbating
polarization in our discourse and in society—potentially leading to poorer
outcomes for broader society.
237, ,294293
“Core discussion networks,” are circles of people who have conversations on
timely but difficult topics such as politics, finances, world events, religion,
health, and more. The nature, size, and diversity of these discussion networks are
important to how individuals form opinions, attitudes, and awareness of differing
perspectives.
295
They ultimately foster political tolerance.
296
Generally, the size
and diversity of core discussion networks have been shrinking substantially
over the recent decades.
297
One survey of 1,055 U.S. adults during the 2016 U.S.
presidential election found that core discussion networks were smaller than in any
other observed period and that the proportion of individuals with the same political
preference within core discussion networks was higher than reported previously.
298
As discussion networks shrink and become more politically homogenous while
society becomes more polarized, it is perhaps not surprising that almost 6 in 10
U.S. adults report that it is “stressful and frustrating” to talk about politics with
people who hold different political opinions.
299
A recent survey found that 64%
of individuals believe that people are incapable of having constructive and civil
debates about issues on which they disagree.
300
Additionally, growing ideological
divisions in the U.S. are fueling skepticism and even animosity between groups
across the political divide —sentiments of enmity and disapproval between
Democrats and Republicans more than doubled between 1994 and 2014.
67
Polarization can lead to identity-based extremism and violence, pointing to the
urgent need to foster social connection across group-based ideological differences
through bridging social capital.
293, ,301294
CHAPTER 3: COMMUNITY HEALTH
K
2
EY D
x
ATA
Growing ideological
divisions in America are
fueling skepticism and
even animosity between
groups across the political
divide: sentiments of
enmity and disapproval
between Democrats and
Republicans more than
doubled between 1994
and 2014.

45Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
A National Strategy
to Advance
Social Connection
Chapter 4
The world is just beginning to recognize the vital
importance of social connection. While the evidence of
the severe consequences of social isolation, loneliness,
and overall social disconnection has been building for
decades, a global pandemic crystallized and accelerated
the urgency for the United States to establish a National
Strategy to Advance Social Connection. Such a strategy not
only recognizes the critical importance of advancing social
connection, but also serves as a commitment to invest in
and take actions establishing that our connection with
others is a core value of this nation.
As this advisory has shown, fulfilling connections are a critical and often
underappreciated contributor to individual and population health and longevity,
safety, prosperity, and well-being. On the other hand, social disconnection
contributes to many poor health outcomes, and even to premature death.
Sadly, around 50% of adults in the U.S. reported being lonely in recent years
1-3
—
and that was even before COVID-19 separated so many of us from our friends,
loved ones, and support systems. Our bonds with others and our community are
also part of this equation. Research has shown that more connected communities
enjoy higher levels of well-being. The converse is also true. How do we put this
important information to practical use in our society? What actionable steps can
we take to enhance social connection so that we can all enjoy its benefits?
A National Strategy to Advance Social Connection is the critical next step to
catalyze action essential to our nation’s health, safety, and prosperity. The strategy
includes six foundational pillars and a series of key recommendations, organized
according to stakeholder group, to support a whole-of-society approach to
advancing social connection. Individuals and organizations can use this framework
to propel the critical work of reversing these worrisome trends and strengthening
social connection and community.

46Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Doing so won’t always be easy. Fostering greater connection requires widespread
individual and institutional action. It demands our sustained investment, effort, and
focus. But it will be worth it, because when we each take these critical steps, we
are choosing better lives, and to create a better world for all.
Such a world, where we recognize that relationships are just as essential to our
well-being as the air we breathe and the food we eat, is a world where everyone
is healthier, physically and mentally. It is a world where we respect and value one
another, where we look out for one another, and where we create opportunities
to uplift one another. A world where our highs are higher because we celebrate
them together; where our lows are more manageable because we respond to them
together; and where our recovery is faster because we grieve and rebuild together.
It is a world where we are strong enough to hold our differences, where we are
more comfortable and motivated to engage civically, and where our leaders and
institutions are more representative of the people they serve. It is a world where
we trust one another, where we feel safe to challenge one another and change
our minds, and where prosperity and progress are not the privilege of the few but
accessible to all.
We can choose, in short, to take the core values that make us strong—love,
kindness, respect, service, and commitment to one another—and reflect them in
the world we build for ourselves and our children. This strategy shows us how to
create the connected lives and the connected world we need.
Benefits of a National Strategy to Advance Social Connection
• Cultivating individual health and well-being across physical and mental health
and educational and economic outcomes. This enables individuals to be happier,
more prosperous, and to contribute more fully to society.
• Strengthening community health, safety, and prosperity by cultivating
social cohesion and social capital within and across communities. This enables
communities to overcome adversity and thrive.
• Building resilience for the next set of challenges such as natural hazards,
pandemics, and safety threats. This enables society to withstand unanticipated
crises through stronger recovery and resilience.
• Advancing civic engagement and representative government by fostering a
more engaged citizenry. This enables policies and programs to better reflect the
will of a community and its individuals.
CHAPTER 4: A NATIONAL STRATEGY

47Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
FIGURE 6: The Six Pillars to Advance Social Connection
CHAPTER 4: A NATIONAL STRATEGY

48Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY
Many factors that influence social connection are environmental. Decisions about
the layout of our cities, from the usability and reach of public transportation to the
design of housing and green spaces, have a direct effect on social interaction in
a community.
302,303
This is why strengthening social infrastructure that promotes
social connection is critical to advancing key aspects of community health,
resilience, safety, and prosperity. Social infrastructure refers to the programs
(such as volunteer organizations, sports groups, religious groups, and member
associations), policies (like public transportation, housing, and education), and
physical elements of a community (such as libraries, parks, green spaces, and
playgrounds) that support the development of social connection.
Investing in local communities and in social infrastructure will fall short if
access to the benefits is limited to only some groups. Equitable access to social
infrastructure for all groups, including those most at-risk for social disconnection,
is foundational to building a connected national and global community, and is
essential to this pillar’s success.
Moreover, community programs, such as those that connect us to our neighbors,
those that help students establish social skills in schools, and those that generate
opportunities for high-risk populations to create community, also have a powerful
role in building relationships. For example, volunteering is a demonstrated and
powerful way to advance connection to one’s community and create diverse ties
among community members. Finally, institutions that gather individuals for work,
study, or prayer, such as workplaces, schools, and faith organizations, can function
as sources of positive connection and thereby bolster the community’s trust in
those institutions and in fellow members. Investing in community connection
will be important to repairing divisions and rebuilding trust in each other and our
institutions, and is vital to achieving common societal goals.
Pillar 1
Strengthen Social Infrastructure
in Local Communities
• Design the built environment to promote social connection
• Establish and scale community connection programs
• Invest in local institutions that bring people together
The Six Pillars
to Advance
Social Connection
49Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY
National, state, local, and tribal governments play a critical role in strengthening
social connection and community across all sectors. These institutions recognize
the importance of social connection to the health of their communities.
Policymakers understand that while the effects of social connection may be most
evident for health, the drivers of connection and disconnection can be found in
all types of policies, from transportation and zoning to nutrition and labor.
A “Connection-in-All-Policies” approach recognizes that every sector of society
is relevant to social connection, and that policy within each sector may potentially
hinder or facilitate connection. Conversely, government has a responsibility to use
its authority to monitor and mitigate the public health harm caused by policies,
products, and services that drive social disconnection.
Prioritizing social connection in policy agendas and leveraging a “Connection-
in-All-Policies” approach requires establishing cross-departmental leadership
to develop and oversee an overarching social connection strategy. Diversity, equity,
inclusion, and accessibility are critical components of any such strategy. It must
recognize that everyone is impacted by social connection, but that some groups
may be more disproportionally impacted by some policies. Thus, policymakers
must give focused attention to reducing disparities in risk and ensuring equal
access to benefits.
Pillar 2
Enact Pro-Connection Public Policies
• Adopt a “Connection-in-All-Policies” approach
• Advance policies that minimize harm from disconnection
• Establish cross-departmental leadership at all levels of government
The Six Pillars
to Advance
Social Connection

50Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY
Social connection is an independent protective factor, and social isolation and
loneliness are independent risk factors for several major health conditions,
including cardiovascular disease, dementia, depression, and premature mortality
from all causes.
128
While all organizations have a role in addressing social
connection, mobilizing the health sector—most notably health care delivery
systems and the public health community—is a core pillar of the National Strategy.
It is critical that we invest in health care provider education on the physical and
mental health benefits of social connection, as well as the risks associated with
social disconnection. We must also create systems that enable and incentivize
health care providers to educate patients as part of preventative care, assess
for social disconnection, and respond to patients’ health-relevant social needs.
This can be accomplished both within the medical system and by linking
individuals to community-based organizations that can provide necessary support
and resources specifically designed to increase social connection.
10, , ,305
304285
Public health organizations can help track the community prevalence of social
disconnection, promote individual best practices, and advance community
solutions. By integrating social connection into primary-, secondary-, and
tertiary-level prevention and care efforts, we can strive to prevent forms of social
disconnection in healthy individuals, mitigate forms of social disconnection early
on before they become severe, and provide adequate support for those who are
experiencing severe forms of social disconnection.
Pillar 3
Mobilize the Health Sector
• Train health care providers
• Assess and support patients
• Expand public health surveillance and interventions
The Six Pillars
to Advance
Social Connection

51Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY
The exponential growth of technology crosses geographic borders, broadening
communities and opening the world to those with limited access. It has had a
tangible impact on how we live and work, from social connectivity, gaming, content
sharing, and virality, to flexible work environments and communication.
But these benefits come at a cost. Technology can also distract us and occupy
our mental bandwidth, make us feel worse about ourselves or our relationships,
and diminish our ability to connect deeply with others. Some technology fans the
flames of marginalization and discrimination, bullying, and other forms of severe
social negativity.
We must decide how technology is designed and how we use it. There are many
ways to minimize harms. We must learn more by requiring data transparency
from technology companies. This will enable us to understand their current
and long-term effects on social connection, and implement and enforce safety
standards (such as age-related protections for young people) that ensure products
do not worsen social disconnection. In a positive vein, we should support the
development of pro-connection technology to promote healthy social connection,
create safe environments for discourse, and safeguard the well-being of users.
This should be coupled with the public’s greater ability to avoid or limit their own uses.
Finally, we need to recognize the unique aspects of digital technology that may
differ from other modes of connecting socially. The modality of delivery matters,
and should be strategically and explicitly acknowledged and evaluated.
Pillar 4
Reform Digital Environments
• Require data transparency
• Establish and implement safety standards
• Support development of pro-connection technologies
The Six Pillars
to Advance
Social Connection
52Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY
This Surgeon General’s Advisory outlines a summary of the evidence about how
social connection and disconnection impact individual and community health and
overall well-being. The totality of this evidence illustrates that urgent action is
needed, including additional research to further advance our understanding of the
causes and consequences of social connection, trends, populations at risk, and the
effectiveness of interventions and other efforts to advance connection.
As a next step, relevant stakeholders, including government, policymakers,
practitioners, and researchers, should work together to establish a research
agenda focused on addressing identified gaps in the evidence base, fund research
at levels commensurate with the seriousness of the problem, and create a plan to
increase research coordination. Deepening our knowledge of social connection
and disconnection also requires us to further refine and expand our capacity
to measure these states via agreed upon standardized metrics. As individuals,
communities, institutions, and governments implement the pillars of the National
Strategy, consistent measurement will be critical to better understanding the
driving forces of connection and disconnection, and how we can be more effective
and efficient in addressing these states.
Public understanding of the essential role of social connection in health and
well-being is critical to this pillar. Social connection should be included as a
key driver of health in formal health education, from elementary to professional
school curricula. It is also imperative that we share this knowledge beyond health
professionals. Public awareness and education of the drivers and solutions of
connection and disconnection will be a critical foundation to support sustained
policy and cultural change.
Pillar 5
Deepen our Knowledge
• Develop and coordinate a national research agenda
• Accelerate research funding
• Increase public awareness
The Six Pillars
to Advance
Social Connection

53Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY
A culture of connection is vital to creating the changes needed in society.
While formal programs and policies can be impactful, the informal practices of
everyday life—the norms and culture of how we engage one another—significantly
influence social connection. These shared beliefs and values drive our individual
and collective behaviors that then shape programs and policies. We cannot be
successful in the other pillars without this underlying culture of connection.
Such a culture of connection rests on core values of kindness, respect, service, and
commitment to one another. Everyone contributes to the collective culture of social
connection by regularly practicing these values. Advancing this culture requires
individuals and leaders to seek opportunities to do so in public and private dialogue,
schools, workplaces, and in the forces that shape our society like media and
entertainment, among others. Behaviors are both learned from and reinforced by
the groups we participate in and the communities we are a part of. Thus, the more
we observe others practicing these values, the more they will be reinforced in us.
All types of leaders and influencers (national, local, political, cultural, corporate,
etc.) can use their voices to underscore these core values and model healthy social
connection and dialogue. Media and entertainment shape our beliefs through the
depiction of stories. These narratives can help individuals see themselves in stories
and help to reduce stigma, thus enabling more connection. Further, our institutions
should invest time, attention, and resources in ways that demonstrate these values.
Pillar 6
Cultivate a Culture of Connection
• Cultivate values of kindness, respect, service, and commitment
to one another
• Model connection values in positions of leadership and influence
• Expand conversations on social connection in schools, workplaces,
and communities
The Six Pillars
to Advance
Social Connection

54Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY
Recommendations for Stakeholders
to Advance Social Connection
All of us as individuals, organizations, and communities can play a role in
increasing and strengthening connection across the nation. This section details
recommendations for how each stakeholder group can take action to advance
social connection.
55 National, Territory, State, Local, and Tribal Governments
56 Health Workers, Health Care Systems, and Insurers
57 Public Health Professionals and Public Health Departments
58 Researchers and Research Institutions
59 Philanthropy
60 Schools and Education Departments
61 Workplaces
62 Community-Based Organizations
63 Technology Companies
64 Media and Entertainment Industries
65 Parents and Caregivers
66 Individuals

55Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY RECOMMENDATIONS FOR STAKEHOLDERS
• Designate social connection a priority by including
it in public health and policy agendas, providing
critical resources, and creating strategies to
strengthen social connection and community that
include clear benchmarks, measurable outcomes,
and periodic evaluation.
• Establish a dedicated leadership position to work
across departments, convene stakeholders, and
advance pro-connection policies.
• Utilize a “Connection-in-All-Policies” Approach
that examines policies across sectors, including
health, education, labor, housing, transportation, and
the environment, and looks to identify and remedy
policies that drive disconnection while advancing
those that drive connection. Periodically, evaluate
and revise existing policies and programs, and when
appropriate, propose new policies to advance social
connection. Examples of pro-connection policies
include paid leave, which enables individuals to
spend time with family during critical early life
stages, and increased access to public transit, which
allows individuals to physically connect more easily.
• Monitor and regulate technology by establishing
transparency, accountability, safety, and consumer
protections to ensure social health and safety
(including for minors) and the ability for independent
researchers to evaluate the impact of technology
on our health and well-being.
306
• Create a standardized national measure or set of
measures for social connection and standardized
definitions for relevant terms, in collaboration with
the research community. Implement consistent,
regular measurement of social connection metrics
in current national health surveys, with the ability
to capture the level of granularity needed to guide
strategic decision-making, planning, and evaluation
of strategies.
• Prioritize research funding such that research is
supported at levels commensurate with the societal
impact of loneliness, social isolation, and other forms
of social disconnection, and enhance collaboration
with researchers to improve research coordination.
• Launch sustained and inclusive public education
and awareness efforts, including the development
of national guidelines for social connection.
307
• Invest in social infrastructure at the local level,
including the programs, policies, and physical
elements of a community that facilitate bringing
people together.
• Incentivize the assessment and integration
of social connection into health care delivery and
public health, including through public insurance
coverage and other government funding mechanisms.
• Increase evaluation and oversight of policy and
programmatic outcomes from public institutions,
programs, and services, and make the results
available through public facing reports, databases,
and other mechanisms. This will help improve
existing policies and programs, demonstrate
transparency, and increase public trust in institutions.
What National, Territory, State, Local,
and Tribal Governments Can Do

56Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY
• Explicitly acknowledge social connection as a
priority for health.
• Provide health professionals with formal training
and continuing education on the health and medical
relevance of social connection and risks associated
with social disconnection (e.g., isolation, loneliness,
low social support, social negativity), as well as
advanced training on prevention and interventions.
• Insurance companies should provide adequate
reimbursement for time spent assessing and
addressing concerns about social disconnection
(e.g., isolation, loneliness, low social support,
poor relationship quality), and incorporate these
measurements into value-based payment models.
• Facilitate inclusion of assessment results in
electronic health records.
• Providers and insurers can educate and incentivize
patients to understand the risks of, and take action
to address, inadequate social connection, with a
particular focus on at-risk individuals, including but
not limited to those with physical or mental health
conditions or disabilities, financial insecurity, those
who live alone, single parents, and both younger and
aging populations.
• Integrate social connection into patient care
in primary-, secondary-, and tertiary-level care
settings by:
⚬
Actively assessing patients’ level of social
connection to identify those who are at increased
risk or already experiencing social disconnection
and evaluate the level of necessary supports.
305
⚬
Educating patients about the benefits of social
connection and the risk factors for social
disconnection as part of primary prevention.
⚬
Leveraging interventions that provide psychosocial
support to patients, including involving family or
other caregivers in treatment, group therapies, and
other evidence-based options.
304
• Work with community organizations to create
partnerships that provide support for people who are
at risk for, or are struggling with, loneliness, isolation,
low social support, or poor-quality relationships.
• Create opportunities for clinicians to partner
with researchers to evaluate the application
of evidence-based assessment tools and
interventions within clinical settings, including
evaluating the efficacy of applications for
specific populations.
10
What Health Workers, Health Care
Systems, and Insurers Can Do
RECOMMENDATIONS FOR STAKEHOLDERS

57Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY
What Public Health Professionals and
Public Health Departments Can Do
• Establish social connection as a priority health
indicator and social determinant of health with
the goal of improving health and well-being
through programs, education, research, and
promotion of healthy lifestyles across the lifespan.
• Develop, lead, and support public education
programs, awareness campaigns, and health
professional training programs focused on the
health impacts of social disconnection. Integrate
social connection as a key component of health
promotion and wellness programs focused on
related health issues (e.g., suicide, workplace
burnout, substance use).
308,309
• Study and support research on the causes
of social disconnection.
RECOMMENDATIONS FOR STAKEHOLDERS
• Evaluate, develop, and implement sustainable
interventions and strategies (e.g., programs,
campaigns, tools, partnerships) across the
social-ecological model to promote greater
connection and prevent social disconnection.
• Consistently and regularly track social connection
using validated metrics (such as the Berkman-Syme
Social Network Index, UCLA Loneliness Scale),
and validate new measures to capture the
full complexity of social connection to guide
strategic decision-making, planning, and
evaluation of strategies.

58Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
• Establish social connection as a research priority
and support researchers in this field with time,
space, and funding.
32
• Develop a cross-disciplinary research agenda
including basic, translational, evaluation,
and dissemination research that prioritizes
systematically mapping outstanding evidence gaps
to ensure adequate evidence across all levels of
the social-ecological model, sectors of society, and
the life course, with attention to inclusion, diversity,
equity, access, and modality considerations. This
research should include investigations into:
⚬
The root causes of social disconnection, including
how causal mechanisms vary across age, income,
culture, race, ethnicity, gender identity, sexual
orientation, and health status to advance equity
in social well-being for all members of the
community, and ensure research is inclusive of
under-represented groups.
10,19
⚬
What social connection indicators may intersect
or act independently, additively, or synergistically
to influence risk and resilience for health
and other societal outcomes.
⚬
Fuller examinations of age, developmental,
and cohort processes that may influence the
onset and progression of disease and other
adverse outcomes.
⚬
Rigorous evaluation of technology’s evolving
impact on social connection.
⚬
The effectiveness, efficiency, and
acceptability of prevention, intervention,
and dissemination approaches.
CHAPTER 4: A NATIONAL STRATEGY
⚬
Additional examinations of individual and societal
effects of social connection within and beyond
health outcomes, including indicators of well-being
(e.g., wider community participation, quality of
life), prosperity (e.g., educational attainment,
employment, economic mobility), and public safety.
• Develop and establish additional standardized
national and local measures that are regularly
evaluated and can be used across basic research,
clinical assessment, population surveillance,
intervention evaluation, and other contexts.
• Improve research coordination, including the
development of an accessible evidence database,
a way to coordinate utilization of evidence among
researchers, and a comprehensive way to track
connection and community metrics over time.
What Researchers and Research
Institutions Can Do
RECOMMENDATIONS FOR STAKEHOLDERS

59Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY
What Philanthropy Can Do
• Fund new programs and invest in existing
successful programs that advance social
connection among individuals and within
communities, including those that aim to prevent
and treat social isolation and loneliness and
those that reach populations at highest risk.
• Because social connection can be advanced through
programs designed to support other outcomes
(e.g., population health, community resilience, public
safety, educational attainment, economic progress)
funders should evaluate cross-sector programs for
their impact on social connection by adding social
connection and relationship-building as indicators
of grantee success.
RECOMMENDATIONS FOR STAKEHOLDERS
• Provide support for adequate evaluation, reporting,
and knowledge sharing about the effectiveness
of interventions designed to reduce loneliness and
isolation and improve social connection.
• Convene stakeholders working to understand
or strengthen social connection.
• Invest in efforts to increase public awareness
and dissemination of findings.

60Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
School administrators and leaders, boards of
education, boards of trustees, teachers, parent
teacher associations, state departments of education,
and online learning platforms can all play a role.
• Develop a strategic plan for school connectedness
and social skills with benchmark tracking.
This could include providing regular opportunities
and spaces for students to develop social skills
and strengthen relationships, and the adoption
of evidenced-based practices leveraging elements
of the CDC Framework: Whole School, Whole
Community, Whole Child.
310
Strategies to enhance
connectedness may include promoting quality
adult support from family and school staff,
peer-led programs, and partnerships with key
community groups.
CHAPTER 4: A NATIONAL STRATEGY
What Schools and Education
Departments Can Do
• Build social connection into health curricula,
including up-to-date, age-appropriate information
on the consequences of social connection
on physical and mental health, key risk and
protective factors, and strategies for increasing
social connection.
• Implement socially based educational techniques
such as cooperative learning projects that
can improve educational outcomes as well as
peer relations.
311
• Create a supportive school environment that
fosters belonging through equitable classroom
management, mentoring, and peer support groups
that allow students to lean on one another and learn
from each other’s experiences.
RECOMMENDATIONS FOR STAKEHOLDERS

61Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
• Make social connection a strategic priority in the
workplace at all levels (administration, management,
and employees).
48
• Train, resource, and empower leaders
and managers to promote connection in the
workplace and implement programs that foster
connection. Assess program effectiveness,
identify barriers to success, and facilitate continuous
quality improvement.
• Leverage existing leadership and employee
training, orientation, and wellness resources to
educate the workforce about the importance
of social connection for workplace well-being,
health, productivity, performance, retention,
and other markers of success.
CHAPTER 4: A NATIONAL STRATEGY
What Workplaces Can Do
RECOMMENDATIONS FOR STAKEHOLDERS
• Create practices and a workplace culture that
allow people to connect to one another as whole
people, not just as skill sets, and that fosters
inclusion and belonging.
• Put in place policies that protect workers’ ability
to nurture their relationships outside work
including respecting boundaries between work
and non-work time, supporting caregiving
responsibilities, and creating a culture of norms
and practices that support these policies.
• Consider the opportunities and challenges posed
by flexible work hours and arrangements (including
remote, hybrid, and in-person work), which may
impact workers’ abilities to connect with others
both within and outside of work. Evaluate how
these policies can be applied equitably across
the workforce.

62Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Community-based organizations include, but are
not limited to, membership-based organizations,
civic groups, arts and education groups, faith-based
organizations, direct service providers, and youth-led
organizations. Regardless of whether the mission of
a community-based organization is focused on social
connection, every organization can promote stronger
social connection.
• Create opportunities and spaces for inclusive
social connection and establish programs that
foster positive and safe relationships, including
among individuals of different ages, backgrounds,
viewpoints, and life experiences.
• Embed social connection in internal policies,
practices, programs, and evaluations.
• Actively seek and build partnerships with
other community institutions (schools, health
organizations, workplaces) to support those
experiencing loneliness and social isolation,
and to create a culture of connection in the
broader community.
CHAPTER 4: A NATIONAL STRATEGY
What Community-Based
Organizations Can Do
• Advance public education and awareness
efforts to introduce and elevate the topic of
social connection and disconnection among
community members.
• Create and provide education, resources, and
support programs for community members and
key populations such as parents, youth, and at-risk
populations. These could include community-wide
social events, volunteering and community
service activities, network-building professional
development, and organizational opportunities
for involvement by the community.
• Foster a culture of connection in the broader
community by highlighting examples of healthy
social connection and leading by example.
RECOMMENDATIONS FOR STAKEHOLDERS

63Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
• Be transparent with data that illustrates both the
positive and negative impacts of technology on
social connection by sharing long-term and real-time
data with independent researchers to enable a
better understanding of technology’s impact on
individuals and communities, particularly those at
higher risk of social disconnection.
• Support the development and enforcement of
industry-wide safety standards with particular
attention to social media, including age-appropriate
protections and identity assurance mechanisms,
to ensure safe digital environments that enable
positive social connection, particularly for minors.
CHAPTER 4: A NATIONAL STRATEGY
What Technology Companies Can Do
RECOMMENDATIONS FOR STAKEHOLDERS
• Intentionally design technology that fosters
healthy dialogue and relationships, including
across diverse communities and perspectives.
The designs should prioritize social health and safety
as the first principle, from conception to launch to
evaluation. This also means avoiding design features
and algorithms that drive division, polarization,
interpersonal conflict, and contribute to unhealthy
perceptions of one’s self and one’s relationships.

64Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
What Media and Entertainment
Industries Can Do
• Create content that models and promotes positive
social interactions, healthy relationships, and
reinforces the core values of connection: kindness,
respect, service, and commitment to one another.
• Utilize storylines and narratives in film, television,
and entertainment to provide messages that broaden
public awareness of the health benefits of social
connection and the risks of social disconnection.
CHAPTER 4: A NATIONAL STRATEGY RECOMMENDATIONS FOR STAKEHOLDERS
• Ensure that content related to social connection
is scientifically accurate in collaboration with the
scientific community.
• Avoid content and products that inadvertently
increase disconnection or stigma around social
disconnection, recognizing the impact content can
have on increasing societal distrust, polarization,
and perpetuating harmful stereotypes.

65Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
CHAPTER 4: A NATIONAL STRATEGY
What Parents and Caregivers Can Do
Parents and caregivers play an important role in
shaping the experience of social connection. Although
focused on parents of young children, many of these
recommendations can apply more broadly to all types
of caregivers.
• Invest in your relationship with your child or loved
one by recognizing that strong, secure attachments
are protective and a good foundation for other
healthy relationships.
• Model healthy social connection, including
constructive conflict resolution, spending time
together, staying in regular contact with extended
family, friends, and neighbors, setting time aside for
socializing away from technology or social media,
and participating in community events.
• Help children and adolescents develop strong,
safe, and stable relationships with supportive
adults like grandparents, teachers, coaches,
counselors, and mentors.
• Encourage healthy social connection with peers
by supporting individual friendships, as well
as participation in structured activities such as
volunteering, sports, community activities,
and mentorship programs.
• Be attentive to how young people spend their time
online. Delay the age at which children join social
media platforms and monitor and decrease screen
time in favor of positive, in-person, connection
building activities.
• Identify and aim to reduce behaviors and
experiences that may increase the risk for social
disconnection, including bullying and excessive
or harmful social media use.
• Talk to your children about social connection
regularly to understand if they are struggling with
loneliness or isolation, to destigmatize talking about
these feelings, and to create space for children to
share their perspective and needs.
⚬
Look out for potential warning signs of loneliness
and social isolation, such as increases in time
spent alone, disproportionate online time,
limited interactions with friends, or excessive
attention-seeking behavior.
312,313
⚬
Connect youth to helpers like counselors, educators,
and health care providers if they are struggling
with loneliness, isolation, or unhealthy relationships.
RECOMMENDATIONS FOR STAKEHOLDERS

66Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
• Understand the power of social connection and the
consequences of social disconnection by learning
how the vital components (structure, function, and
quality) can impact your relationships, health, and
well-being.
• Invest time in nurturing your relationships through
consistent, frequent, and high-quality engagement
with others. Take time each day to reach out to a
friend or family member.
• Minimize distraction during conversation to
increase the quality of the time you spend with
others. For instance, don’t check your phone during
meals with friends, important conversations, and
family time.
• Seek out opportunities to serve and support others,
either by helping your family, co-workers, friends,
or strangers in your community or by participating
in community service.
• Be responsive, supportive, and practice
gratitude.
314,315
As we practice these behaviors,
others are more likely to reciprocate, strengthening
our social bonds, improving relationship satisfaction,
and building social capital.
• Actively engage with people of different
backgrounds and experiences to expand your
understanding of and relationships with others, given
the benefits associated with diverse connections.
• Participate in social and community groups such
as fitness, religious, hobby, professional, and
community service organizations to foster a sense
of belonging, meaning, and purpose.
CHAPTER 4: A NATIONAL STRATEGY
• Reduce practices that lead to feelings of
disconnection from others. These include harmful
and excessive social media use, time spent in
unhealthy relationships, and disproportionate time
in front of screens instead of people.
• Seek help during times of struggle with loneliness
or isolation by reaching out to a family member,
friend, counselor, health care provider, or the 988
crisis line.
316
• Be open with your health care provider about
significant social changes in your life, as this may
help them understand potential health impacts and
guide them to provide recommendations to mitigate
health risks.
• Make time for civic engagement. This could include
being a positive and constructive participant in
political discourse and gatherings (e.g., town halls,
school board meetings, local government hearings).
• Reflect the core values of connection in how you
approach others in conversation and through the
actions you take. Key questions to ask yourself when
considering your interactions with others include:
How might kindness change this situation?
What would it look like to treat others with respect?
How can I be of service? How can I reflect my
concern for and commitment to others?
RECOMMENDATIONS FOR STAKEHOLDERS
What Individuals Can Do

67Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Hundreds of independent studies across several scientific disciplines have
examined the objective physical and mental health outcomes of social connection,
social isolation, and loneliness for individuals.
10
Despite the variability in conceptual
and methodological approaches used in the research, these findings converge
to demonstrate a robust and reliable association between social connection and
health outcomes.
37, , , ,318317128127
In addition to significant evidence of correlations between social connection and
health, evidence supports a potential causal association. Using the Bradford Hill
Guidelines,
58,131
as well as some newer studies leveraging causal epidemiology
319-323
and experimental evidence in animals,
324,325
together suggests a likely causal
association between social isolation and a variety of poor health outcomes,
including death. In humans, experimental evidence and intervention-based
studies using randomized controlled trials also supports the likelihood of a causal
association between broader social connection and better health and longer
life expectancy.
304
Importantly, there is evidence of a dose-response relationship between social
connection and health.
59
This means that incremental increases in social
connection correspond to decreases in risk to health, and conversely, decreases
in social connection correspond to increases in risk. Evidence demonstrates this
dose-response relationship exists for developmental stages across the lifespan,
suggesting that social connection is a continuum from risk (when low) to protection
(when high). This suggests social connection is relevant to all humans regardless
of our individual positions along the risk trajectory.
Despite the strength of the evidence linking social connection to various health
outcomes, certain gaps and limitations in research still exist. For example,
few studies examine more than one social connection component (structural,
functional, and quality indicators) in the same sample to disentangle the
independent, additive, and synergistic effects. This complicates the measurement
of an individual’s risk associated with lack of social connection (e.g., social isolation,
loneliness, social negativity) and confounds the understanding of the unique
and complex pathways by which social connection influences health. Further,
despite significant changes in the way in which we interact socially, many research
studies do not distinguish remote or technology-mediated social connection from
traditional means of connecting socially to determine equivalencies and to discern
the influence on long-term health and mortality risk. Yet, despite these challenges,
the extensive and replicated body of existing evidence offers a compelling basis
for elevating the discourse on promoting social connection and addressing social
disconnection with targeted public health policies, initiatives, and actions.
Strengths and Limitations
of the Evidence

68Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
STRENGTHS AND LIMITATIONS OF THE EVIDENCE
In regard to the study of community-level benefits, significant differences exist
in how researchers approach community-level social connection across scientific
studies. For instance, variations exist in the indicators researchers use to define
and measure social connection. While social cohesion, social capital, belonging,
and trust are all indicators of connected communities, many studies examine only
one of these concepts and few examine all of these to disentangle their relative
influence or relate them directly to loneliness and isolation. Complicating matters,
some studies also use different terms to refer to the same concept or use the same
term to refer to different concepts. Much of this research is correlative in nature
and necessitates further study, including among often underrepresented groups,
in order to understand causative factors that produce community-level benefits.
Another layer of complexity is how different each community is along a multitude
of dynamics and factors such as policies, customs, cultures, assets, challenges,
demographics, and more. This variation means there is no “one-size-fits-all”
approach to community connection, and it means that different communities will
have different needs and desires. Despite all of these differences and complexities,
there is strong evidence that points to social connection as an important factor in
strengthening communities and community-level outcomes. While more research is
needed, the evidence we do have suggests that enhancing community connection
may help us address many important community and societal issues.

69Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Lead Science Editor
Julianne Holt-Lunstad, PhD
Professor of Psychology and Neuroscience, Brigham Young University,
and Director, Social Connections Lab. Scientific Chair and Board Member,
Foundation for Social Connection, and Global Initiative on Loneliness
and Connection
Copy Editor
Susan Golant, MA
Writer and Editor
Department of Health and Human Services (HHS)
Administration for Children and Families (ACF)
Administration for Community Living (ACL)
Agency for Healthcare Research and Quality (AHRQ)
Centers for Disease Control and Prevention (CDC)
Office of the Director
Division of Adolescent and School Health
Division of Population Health
Centers for Medicare and Medicaid Services (CMS)
Health Resources and Services Administration (HRSA)
Indian Health Service (IHS)
National Institutes of Health (NIH)
Office of the Assistant Secretary for Health (OASH)
Office of the Assistant Secretary for Planning and Evaluation (ASPE)
Office of the General Counsel (OGC)
Substance Abuse and Mental Health Services Administration (SAMHSA)
Acknowledgments
Our Epidemic of Loneliness and
Isolation: The Surgeon General’s
Advisory on the Healing Effects of
Social Connection and Community
was prepared by the Office of the
Surgeon General with valuable
contributions from partners
across the U.S. Government and
external reviewers, including,
but not limited to:

70Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
Reviewers
The Office of the Surgeon
General solicited an independent
review of the advisory or
selected sections in draft
form. Reviewers were selected
for their technical expertise,
and they provided individually
many constructive comments.
The below reviewers did not
view a final version of the
advisory prior to its release,
nor were they asked to
endorse the conclusions or
recommendations. We thank
the following individuals for
their review of the advisory:
ACKNOWLEDGMENTS
Juan R. Albertorio-Diaz, MA,
Statistician, National Center for Health
Statistics, Centers for Disease Control
and Prevention. Senior Research Advisor,
Foundation for Social Connection.
Daniel P. Aldrich, PhD, Co-Director,
Global Resilience Institute, and Director,
Security and Resilience Studies Program.
Professor, Political Science and Public
Policy, Northeastern University.
Ursula Bauer, PhD, MPH, Deputy
Commissioner for Public Health
and Director, Office of Public Health,
New York State Department of Health.
Lauren Behsudi, Senior Advisor,
Administration for Children and Families.
Andrew Breeden, PhD, Program Chief,
Social and Affective Neuroscience
Program, Division of Neuroscience and
Basic Behavioral Science, National
Institute of Mental Health.
Katherine V. Bruss, PsyD, Mental Health
Lead, Division of Population Health,
National Center for Chronic Disease
Prevention and Health Promotion, Centers
for Disease Control and Prevention.
Paul Cann, MA, (Cambridge University)
OBE, Co-founder, UK Campaign to End
Loneliness.
Chia-Chia Chang, MPH, MBA,
Coordinator, Office for Total Worker
Health® Collaborations and New
Opportunity Development, and
Co-Coordinator, Healthy Work Design
and Well-Being Cross Sector Program,
National Institute for Occupational
Safety and Health, Centers for Disease
Control and Prevention.
Katie Clark, Policy Analyst, Office
of Integrated Programs and Office
of Network Advancement, Center
for Innovation and Partnership, the
Administration for Community Living.
Thomas K.M. Cudjoe, MD, MPH,
Assistant Professor of Medicine,
Department of Medicine, Division of
Geriatric Medicine and Gerontology,
Johns Hopkins University School
of Medicine. Scientific Advisory
Council Member, Foundation for
Social Connection.
Munmun DeChoudhury, PhD,
Associate Professor, School of
Interactive Computing,
Georgia Institute of Technology.
Dona M. Dmitrovic, MHS, Senior
Advisor, Office of Recovery, Substance
Abuse and Mental Health Services
Administration, U.S. Department of
Health and Human Services.
Felton James (Tony) Earls, MD,
Professor of Social Medicine, Emeritus,
Harvard Medical School. Professor of
Human Behavior and Development,
Emeritus, Harvard T.H. Chan School of
Public Health.
Jesse Ellis, MS, MPA, Prevention
Manager, Fairfax County Department
of Neighborhood and Community
Services, Virginia.
Nicole B. Ellison, PhD, Karl E. Weick
Collegiate Professor of Information,
School of Information, University
of Michigan. Scientific Advisory
Council Member, Foundation for
Social Connection.
Linda Fried, PhD, Dean, Columbia
University Mailman School of Public
Health. Director, Robert N. Butler
Columbia Aging Center.
Edward Garcia III, MHS-PH, Founder
and Board Chair, Foundation for Social
Connection. Co-Founder and Board
Member, Global Initiative on Loneliness
and Connection.
Lori Gerhard, Director of the Office
of Integrated Programs, Center for
Innovation and Partnership, the
Administration for Community Living.

71Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
REVIEWERSACKNOWLEDGMENTS
Jonathan Gruber, Strategy Lead -
Building, Einhorn Collaborative.
Jonathan Haidt, PhD, Professor of
Ethical Leadership, New York University
Stern School of Business.
Hahrie Han, PhD, Stavros Niarchos
Foundation Professor of Political Science,
and Inaugural Director, SNF Agora
Institute, Johns Hopkins University.
Debra Houry, MD, MPH, Chief Medical
Officer and Deputy Director for
Program and Science, Centers for
Disease Control and Prevention.
Maggie Jarry, MDiv, MS, Senior
Emergency Management Specialist,
Substance Abuse and Mental Health
Services Administration, U.S. Department
of Health and Human Services.
Dilip Jeste, MD, Former Senior Associate
Dean for Healthy Aging and Senior
Care, University of California, San Diego.
David I. Leitman, PhD, Program Chief,
Social Neuroscience and Communication
in Adult Psychopathology Program,
Translational Research Division, National
Institute of Mental Health.
Peter Levine, PhD, Lincoln Filene
Professor and Associate Dean, Tisch
College of Civic Life, Tufts University.
Erin McDonald, PhD, MPP, Senior
Advisor and Lead, Equitable Long-Term
Recovery and Resilience Plan, U.S.
Department of Health and Human
Services, Office of the Assistant
Secretary of Health, Office of Disease
Prevention and Health Promotion.
Melissa C. Mercado, PhD, MSc, MA,
Lead Behavioral Scientist, Youth Violence
and Emerging Topics, Division of Violence
Prevention, National Center for Injury
Prevention and Control, Centers for
Disease Control and Prevention.
Christopher Mikton, PhD, Technical
lead on social connection, Department
of Social Determinants of Health, World
Health Organization.
Kathleen Mullan Harris, PhD, James
E. Haar Distinguished Professor of
Sociology, Fellow, Carolina Population
Center, University of North Carolina at
Chapel Hill.
Phyllis Holditch Niolon, PhD, Senior
Scientist for Preventing Adverse
Childhood Experiences, Division of
Violence Prevention, National Center
for Injury Prevention and Control, Centers
for Disease Control and Prevention.
Yolanda Ogbolu, PhD, CRNP, FNAP,
FAAN, Associate Professor, tenured,
Department Chair, Partnerships,
Professional Education and Practice,
Co-Director Center for Health Equity
and Outcomes Research, University of
Maryland Baltimore.
Anthony D. Ong, PhD, Professor of
Psychology, Cornell University.
Professor of Gerontology in Medicine,
Weill Cornel Medicine.
Matthew S. Pantell, MD, MS, Assistant
Professor, Division of Pediatric Hospital
Medicine, Department of Pediatrics,
Center for Health and Community,
University of California, San Francisco.
Scientific Advisory Council Member,
Foundation for Social Connection.
Carla M. Perissinotto, MD, MHS,
Professor of Medicine, Geriatrics,
University of California, San Francisco.
Scientific Advisory Council Member,
Foundation for Social Connection.
Brian A. Primack, MD, PhD, Dean,
College of Public Health and Human
Sciences, Oregon State University.
Robert D. Putnam, PhD, Emeritus
Professor, Harvard Kennedy School.
Jillian Racoosin, MPH, Executive Director,
Foundation for Social Connection.
Harry T. Reis, PhD, Dean’s Professor
in Arts, Sciences, and Engineering,
and Professor of Psychology, University
of Rochester. Scientific Advisory
Council Member, Foundation for
Social Connection.
Joshua Seidman, PhD, Chief Research
and Knowledge Officer, Fountain House.
Christine Sinsky, MD, MACP, Vice
President, Professional Satisfaction,
American Medical Association.
Matthew Lee Smith, PhD, MPH, School
of Public Health, Texas A&M University.
Scientific Advisory Council Member,
Foundation for Social Connection.
Andrew Steptoe, DSc, Professor
of Psychology and Epidemiology,
University College London, London, UK.
Deb Stone, ScD, MSW, MPH, Lead
Behavioral Scientist, Suicide Prevention
Team, National Center for Injury
Prevention and Control, Centers
for Disease Control and Prevention.
Craig W. Thomas, PhD, Director,
Division of Population Health, National
Center for Chronic Disease Prevention
and Health Promotion, Centers for
Disease Control and Prevention.
Bert N. Uchino, PhD, Professor,
Department of Psychology and Health
Psychology Program, University of Utah.
Mark J. Van Ryzin, PhD, Research
Associate Professor, University of Oregon.
Scientific Advisory Council Member,
Foundation for Social Connection.
Laura E. Welder, DrPH, MPH,
Behavioral Scientist, Division of Injury
Prevention, National Center for Injury
Prevention and Control, Centers for
Disease Control and Prevention.
Tia Taylor Williams, MPH, CNS, Director,
Center for Public Health Policy, Center
for School, Health and Education,
American Public Health Association.

72Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
References
1. Cigna Corporation. The Loneliness Epidemic Persists: A Post-
Pandemic Look at the State of Loneliness among U.S. Adults. 2021.
2. Bruce LD, Wu JS, Lustig SL, Russell DW, Nemecek DA. Loneliness
in the United States: A 2018 National Panel Survey of Demographic,
Structural, Cognitive, and Behavioral Characteristics. Am J Health
Promot. 2019;33(8):1123-1133.
3. Shovestul B, Han J, Germine L, Dodell-Feder D. Risk factors
for loneliness: The high relative importance of age versus other
factors. PLOS ONE. 2020;15.
4. Holt-Lunstad J, Robles TF, Sbarra DA. Advancing social
connection as a public health priority in the United States. Am
Psychol. 2017;72(6):517-530.
5. Allen KA, Kern ML, Rozek CS, McInereney D, Slavich GM.
Belonging: A Review of Conceptual Issues, an Integrative
Framework, and Directions for Future Research. Aust J Psychol.
2021;73(1):87-102.
6. Sampson RJ, Raudenbush SW, Earls F. Neighborhoods and
Violent Crime: A Multilevel Study of Collective Efficacy. Science.
1997;277(5328):918-924.
7. Riess H. The Science of Empathy. Journal of Patient Experience.
2017;4(2):74-77.
8. Hu T, Zheng X, Huang M. Absence and Presence of Human
Interaction: The Relationship Between Loneliness and Empathy.
Frontiers in Psychology. 2020;11.
9. Prohaska T, Burholt V, Burns A, et al. Consensus statement:
loneliness in older adults, the 21st century social determinant of
health? BMJ Open. 2020;10(8):e034967.
10. National Academies of Sciences Engineering and Medicine
(NASEM). Social Isolation and Loneliness in Older Adults:
Opportunities for the Health Care System. Washington, DC: The
National Academies Press; 2020.
11. House BR. How do social norms influence prosocial
development? Current Opinion in Psychology. 2018;20:87-91.
12. Putnam RD. Bowling Alone: America’s Declining Social Capital.
In: Crothers L, Lockhart C, eds. Culture and Politics: A Reader. New
York: Palgrave Macmillan US; 2000:223-234.
13. Moore S, Kawachi I. Twenty years of social capital and health
research: a glossary. J Epidemiol Community Health. 2017;71(5):513-517.
14. Bourdieu P. The Forms of Capital. In: Readings in Economic
Sociology. 2002:280-291.
15. National Research Council. Civic Engagement and Social
Cohesion: Measuring Dimensions of Social Capital to Inform Policy.
Washington, DC: The National Academies Press; 2014.
16. Kawachi I, Berkman L. Social Cohesion, Social Capital,
and Health. In: Berkman L, Kawachi I, Glymour M, eds. Social
Epidemiology. Second ed. New York City: Oxford University Press;
2014:174-190.
17. Ehsan A, Klaas HS, Bastianen A, Spini D. Social capital and
health: A systematic review of systematic reviews. SSM - Population
Health. 2019;8:100425.
18. Office of Disease Prevention and Health Promotion, Office of
the Assistant Secretary for Health. Social Cohesion. Office of the
Secretary, U.S. Department of Health and Human Services. https://
health.gov/healthypeople/priority-areas/social-determinants-
health/literature-summaries/social-cohesion. Published 2023.
Accessed April 2023.
19. Badcock JC, Holt-Lunstad J, Bombaci P, Garcia E, Lim MH.
Position statement: addressing social isolation and loneliness and
the power of human connection. Global Initiative on Loneliness and
Connection (GILC).2022.
20. Holt-Lunstad J. Why Social Relationships Are Important for
Physical Health: A Systems Approach to Understanding and
Modifying Risk and Protection. Annu Rev Psychol. 2018;69:437-458.
21. Holt-Lunstad J, Steptoe A. Social isolation: An underappreciated
determinant of physical health. Curr Opin Psychol. 2021;43:232-237.
22. Brooks KP, Dunkel Schetter C. Social negativity and health:
Conceptual and measurement issues. Social and Personality
Psychology Compass. 2011;5(11):904-918.
23. Berkman LF, Glass T, Brissette I, Seeman TE. From social
integration to health: Durkheim in the new millennium. Social
Science & Medicine. 2000;51(6):843-857.
24. Legros S, Cislaghi B. Mapping the Social-Norms Literature:
An Overview of Reviews. Perspectives on Psychological Science.
2020;15(1):62-80.
25. Reid AE, Cialdini RB, Aiken LS. Social norms and health behavior.
In: Handbook of behavioral medicine. Springer; 2010:263-274.
26. Piškur B, Daniëls R, Jongmans MJ, et al. Participation and social
participation: are they distinct concepts? Clinical Rehabilitation.
2013;28(3):211-220.
27. Levasseur M, Richard L, Gauvin L, Raymond A. Inventory and
analysis of definitions of social participation found in the aging
literature: Proposed taxonomy of social activities. Social Science &
Medicine. 2010;71(12):2141-2149.
28. Cohen S, Wills TA. Stress, social support, and the buffering
hypothesis. Psychological Bulletin. 1985;98:310-357.
29. Spadaro G, Gangl K, Van Prooijen J-W, Van Lange PA, Mosso
CO. Enhancing feelings of security: How institutional trust
promotes interpersonal trust. PloS one. 2020;15(9):e0237934.
30. Rotter JB. A new scale for the measurement of interpersonal
trust. Journal of Personality. 1967;35:651-665.
31. Gilson L. Trust and the development of health care as a social
institution. Soc Sci Med. 2003;56(7):1453-1468.
32. Holt-Lunstad J. Social Connection as a Public Health Issue: The
Evidence and a Systemic Framework for Prioritizing the “Social”
in Social Determinants of Health. Annual Review of Public Health.
2022;43(1):193-213.
33. John S. and James L. Knight Foundation, Gallup Inc. Knight Soul
of the Community 2010. 2010.
34. Aldrich DP, Meyer MA. Social capital and community resilience.
American behavioral scientist. 2015;59(2):254-269.
35. Aldrich, Daniel. (2012). Building Resilience: Social Capital in
Post-Disaster Recovery. 10.7208/chicago/9780226012896.001.0001.

73Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
36. United States Department of Health and Human Services.
Community health and economic prosperity: Engaging businesses
as stewards and stakeholders – A report of the Surgeon General.
Atlanta, GA: U.S. Department of Health and Human Services,
Centers for Disease Control and Prevention, Office of the Associate
Director for Policy and Strategy; 2021.
37. Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D.
Loneliness and social isolation as risk factors for mortality: a meta-
analytic review. Perspect Psychol Sci. 2015;10(2):227-237.
38. Valtorta NK, Kanaan M, Gilbody S, Ronzi S, Hanratty B.
Loneliness and social isolation as risk factors for coronary heart
disease and stroke: systematic review and meta-analysis of
longitudinal observational studies. Heart. 2016;102(13):1009-1016.
39. Mann F, Wang J, Pearce E, et al. Loneliness and the onset
of new mental health problems in the general population. Soc
Psychiatry Psychiatr Epidemiol. 2022;57(11):2161-2178.
40. Penninkilampi R, Casey AN, Singh MF, Brodaty H. The
Association between Social Engagement, Loneliness, and Risk of
Dementia: A Systematic Review and Meta-Analysis. J Alzheimers
Dis. 2018;66(4):1619-1633.
41. Lazzari C, Rabottini M. COVID-19, loneliness, social isolation and
risk of dementia in older people: a systematic review and meta-analysis
of the relevant literature. Int J Psychiatry Clin Pract. 2021:1-12.
42. Cohen S. Psychosocial Vulnerabilities to Upper
Respiratory Infectious Illness: Implications for Susceptibility
to Coronavirus Disease 2019 (COVID-19). Perspect Psychol Sci.
2020:1745691620942516.
43. Flowers L, Houser A, Noel-Miller C, et al. Medicare Spends More
on Socially Isolated Older Americans. Washington, D.C.: AARP Public
Policy Institute; 2017.
44. Guay F, Boivin M, Hodges EVE. Predicting change in academic
achievement: A model of peer experiences and self-system
processes. Journal of Educational Psychology. 1999;91:105-115.
45. Maher BM, Hynes H, Sweeney C, et al. Medical School
Attrition-Beyond the Statistics A Ten Year Retrospective Study.
BMC Medical Education. 2013;13(1):13.
46. Bowers A, Wu J, Lustig S, Nemecek D. Loneliness influences
avoidable absenteeism and turnover intention reported by adult
workers in the United States. Journal of Organizational Effectiveness:
People and Performance. 2022;9(2):312-335.
47. Ozcelik H, Barsade SG. No Employee an Island: Workplace
Loneliness and Job Performance. Academy of Management Journal.
2018;61(6):2343-2366.
48. United States Department of Health and Human Services.
The U.S. Surgeon General’s Framework for Workplace Mental Health
and Well-being. Washington, D.C.: U.S. Department of Health and
Human Services, Office of the U.S. Surgeon General; 2022.
49. Morenoff J, Sampson R, Raudenbush S. Neighborhood
Inequality, Collective Efficacy, and the Spatial Dynamics of Urban
Violence Criminology. 2001;39(3):517-558.
50. Kim M, Cho M. Examining the role of sense of community:
Linking local government public relationships and community-
building. Public Relations Review. 2019.
51. Tomova L, Tye K, Saxe R. The neuroscience of unmet social
needs. Soc Neurosci. 2021;16(3):221-231.
52. Coan JA, Sbarra DA. Social Baseline Theory: The Social
Regulation of Risk and Effort. Curr Opin Psychol. 2015;1:87-91.
53. Gallup Inc., Meta. The State of Social Connections. Washington
D.C.: Gallup Inc.,; 2022.
54. Office on Smoking and Health National Center for Chronic
Disease Prevention and Health Promotion. Current Cigarette
Smoking Among Adults in the United States. https://www.cdc.gov/
tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/
index.htm#:~:text=Cigarette%20smoking%20remains%20
the%20leading,about%201%20in%205%20deaths.&text=In%20
2020%2C%20nearly%2013%20of,12.5%25)%20currently*%20
smoked%20cigarettes. Published 2022. Accessed April 2023.
55. Centers for Disease Control and Prevention. Prevalence of Both
Diagnosed and Undiagnosed Diabetes. Centers for Disease Control
and Prevention. https://www.cdc.gov/diabetes/data/statistics-
report/diagnosed-undiagnosed-diabetes.html. Published 2022.
Accessed April 2023.
56. Division of Nutrition Physical Activity and Obesity, National
Center for Chronic Disease Prevention and Health Promotion. Adult
Obesity Facts. Centers for Disease Control and Prevention. https://
www.cdc.gov/obesity/data/adult.html. Published 2022. Accessed
April 2023.
57. DiJulio B, Hamel L, Muñana C, Brodie M. Loneliness and Social
Isolation in the United States, the United Kingdom, and Japan: An
International Survey. 2018.
58. Holt-Lunstad J. The Major Health Implications of Social
Connection. Current Directions in Psychological Science.
2021;30(3):251-259.
59. Yang YC, Boen C, Gerken K, Li T, Schorpp K, Harris KM. Social
relationships and physiological determinants of longevity across
the human life span. Proc Natl Acad Sci U S A. 2016;113(3):578-583.
60. Cacioppo JT, Cacioppo S, Boomsma DI. Evolutionary
mechanisms for loneliness. Cognition & emotion. 2014;28(1):3-21.
61. Coplan RJ, Bowker JC, Nelson LJ. The handbook of solitude:
Psychological perspectives on social isolation, social withdrawal, and
being alone. John Wiley & Sons; 2021.
62. Steptoe A, Shankar A, Demakakos P, Wardle J. Social isolation,
loneliness, and all-cause mortality in older men and women. Proc
Natl Acad Sci U S A. 2013;110(15):5797-5801.
63. Stokes AC, Xie W, Lundberg DJ, Glei DA, Weinstein MA.
Loneliness, social isolation, and all-cause mortality in the United
States. SSM-mental health. 2021;1:100014.
64. Kannan V, Veazie P. US trends in social isolation, social
engagement, and companionship —nationally and by age, sex,
race/ethnicity, family income, and work hours, 2003–2020. SSM -
Population Health. 2023;Volume 21.
65. Putnam RD. The Upswing: How America Came Together a Century
Ago and How We Can Do It Again.: Simon & Schuster; 2020.
REFERENCES

74Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
66. Davern M, Bautista R, Freese J, Morgan S, Smith T. General
Social Surveys, 1972-2021 Cross-section [machine-readable data
file, 68,846 cases]. In: NORC at the University of Chicago, ed.
Chicago: NORC at the University of Chicago,.
67. Pew Research Center. Political Polarization in the American
Public. 2014.
68. Cox D. The State of American Friendship: Change, Challenges,
and Loss. Survey Center on American Life; 2021.
69. Kovacs B, Caplan N, Grob S, King M. Social Networks
and Loneliness During the COVID-19 Pandemic. Socius.
2021;7:2378023120985254.
70. Census Bureau Releases New Estimates on America’s Families
and Living Arrangements [reports]. United States Census Bureau
2022.
71. Atwell M, Stillerman B, Bridgeland JM. Health Index 2021:
Citizenship During Crisis. Civic, National Conference on Citizenship,
University of Virginia’s Miller Center, Democracy Initiative and the
Partnership for American Democracy; 2021.
72. Parker K, Horowitz J, Brown A, Fry R, Cohn D, Igielnik R. What
Unites and Divides Urban, Suburban and Rural Communities. Pew
Research Center; 2018.
73. Pew Research Center. America’s Changing Religious Landscape.
Pew Research Center; 2015.
74. Hout M, Smith TW. Fewer Americans Affiliate with Organized
Religions, Belief and Practice Unchanged. In:2015.
75. Jones JM. US church membership falls below majority for first
time. Gallup News. 2021.
76. Putnam RD, Campbell DE. American Grace: How Religion Divides
and Unites Us. Simon & Schuster; 2010.
77. VanderWeele TJ. Religious communities and human flourishing.
Current Directions in Psychological Science. 2017;26:476-481.
78. Koenig H, Koenig HG, King D, Carson VB. Handbook of religion
and health. Oup Usa; 2012.
79. Office of Disease Prevention and Health Promotion. Social
Determinants of Health. U.S. Department of Health and Human
Services. Healthy People 2030 Web site. https://health.gov/
healthypeople/objectives-and-data/social-determinants-health.
Published n.d. Accessed April 2023.
80. National Center for Injury Prevention and Control, Division of
Violence Prevention. The Social-Ecological Model: A Framework
for Prevention. Centers for Disease Control and Prevention. https://
www.cdc.gov/violenceprevention/about/social-ecologicalmodel.
html. Published 2022. Accessed April 2023.
81. Henry D, Gorman-Smith D, Schoeny M, Tolan P. “Neighborhood
matters”: Assessment of neighborhood social processes. American
Journal of Community Psychology. 2014;54:187-204.
82. Lenzi M, Vieno A, Santinello M, Perkins DD. How neighborhood
structural and institutional features can shape neighborhood social
connectedness: a multilevel study of adolescent perceptions. Am J
Community Psychol. 2013;51(3-4):451-467.
REFERENCES
83. O’Sullivan R, Burns A, Leavey G, et al. Impact of the COVID-19
Pandemic on Loneliness and Social Isolation: A Multi-Country
Study. International Journal of Environmental Research and Public
Health. 2021;18(19):9982.
84. Buecker S, Mund M, Chwastek S, Sostmann M, Luhmann M. Is
loneliness in emerging adults increasing over time? A preregistered
cross-temporal meta-analysis and systematic review. Psychological
Bulletin. 2021;147(8):787.
85. Pew Research Center. Internet/Broadband Fact Sheet. 2021.
86. Roser M, Ritchie H, Ortiz-Ospin E. Internet. Our World in Data. 2015.
87. Perrin M, Atske S. About three-in-ten U.S. adults say they are
‘almost constantly’ online. Pew Research Center; 2021.
88. Vogels E, Gelles-Watnick R, Massarat N. Teens, Social Media
and Technology 2022. Pew Research Center; 2022.
89. Ortiz-Ospina E. The rise of social media. Our World in Data. 2019.
90. Perrin A, Atske S. Americans with disabilities less likely than
those without to own some digital devices. Pew Research Center; 2021.
91. Vogels E. Digital divide persists even as Americans with lower
incomes make gains in tech adoption. Pew Research Center; 2021.
92. Vogels E. Some digital divides persist between rural, urban and
suburban America. Pew Research Center; 2021.
93. Liu D, Ainsworth SE, Baumeister RF. A meta-analysis of social
networking online and social capital. Review of General Psychology.
2016;20(4):369-391.
94. Domahidi E. The associations between online media use and
users’ perceived social resources: A meta-analysis. Journal of
Computer-Mediated Communication. 2018;23(4):181-200.
95. Liu D, Wright KB, Hu B. A meta-analysis of Social Network Site
use and social support. Computers & Education. 2018;127:201-213.
96. Hancock J, Liu SX, Luo M, Mieczkowski H. Psychological
Well-Being and Social Media Use: A Meta-Analysis of Associations
between Social Media Use and Depression, Anxiety, Loneliness,
Eudaimonic, Hedonic and Social Well-Being. Anxiety, Loneliness,
Eudaimonic, Hedonic and Social Well-Being (March 9, 2022). 2022.
97. Uhls YT, Ellison NB, Subrahmanyam K. Benefits
and costs of social media in adolescence. Pediatrics.
2017;140(Supplement_2):S67-S70.
98. Valkenburg PM, Peter J. Online communication among
adolescents: An integrated model of its attraction, opportunities,
and risks. Journal of adolescent health. 2011;48(2):121-127.
99. Yau JC, Reich SM. Are the qualities of adolescents’ offline
friendships present in digital interactions? Adolescent Research
Review. 2018;3(3):339-355.
100. Taylor SH, Zhao P, Bazarova NN. Social media and close
relationships: a puzzle of connection and disconnection. Current
Opinion in Psychology. 2021.
101. Ahmad Z, Soroya SH, Mahmood K. Bridging social capital
through the use of social networking sites: A systematic literature
review. Journal of Human Behavior in the Social Environment. 2022:1-17.

75Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
102. Noone C, McSharry J, Smalle M, et al. Video calls for reducing
social isolation and loneliness in older people: a rapid review.
Cochrane Database Syst Rev. 2020;5(5):Cd013632.
103. Charalampous M, Grant CA, Tramontano C, Michailidis E.
Systematically reviewing remote e-workers’ well-being at work:
a multidimensional approach. European Journal of Work and
Organizational Psychology. 2019;28(1):51-73.
104. Griffiths KM, Calear AL, Banfield M. Systematic review on
Internet Support Groups (ISGs) and depression (1): Do ISGs reduce
depressive symptoms? J Med Internet Res. 2009;11(3):e40.
105. Pandya A, Lodha P. Social Connectedness, Excessive Screen
Time During COVID-19 and Mental Health: A Review of Current
Evidence. Frontiers in Human Dynamics. 2021;3.
106. Sen K, Prybutok G, Prybutok V. The use of digital technology
for social wellbeing reduces social isolation in older adults: A
systematic review. SSM - Population Health. 2022;17:101020.
107. Park PS, Blumenstock JE, Macy MW. The strength of
long-range ties in population-scale social networks. Science.
2018;362(6421):1410-1413.
108. Duplaga M, Szulc K. The Association of Internet Use with
Wellbeing, Mental Health and Health Behaviours of Persons with
Disabilities. Int J Environ Res Public Health. 2019;16(18).
109. Hunt MG, Marx R, Lipson C, Young J. No More FOMO: Limiting
Social Media Decreases Loneliness and Depression. Journal of
Social and Clinical Psychology. 2018;37(10):751-768.
110. Duke É, Montag C. Smartphone addiction, daily interruptions and
self-reported productivity. Addictive Behaviors Reports. 2017;6:90-95.
111. Dwyer RJ, Kushlev K, Dunn EW. Smartphone use undermines
enjoyment of face-to-face social interactions. Journal of
Experimental Social Psychology. 2018;78:233-239.
112. Kushlev K, Dunn EW. Smartphones distract parents from
cultivating feelings of connection when spending time with
their children. Journal of Social and Personal Relationships.
2018;36(6):1619-1639.
113. Misra S, Cheng L, Genevie J, Yuan M. The iPhone Effect: The
Quality of In-Person Social Interactions in the Presence of Mobile
Devices. Environment and Behavior. 2014;48(2):275-298.
114. Primack BA, Shensa A, Sidani JE, et al. Social Media Use and
Perceived Social Isolation Among Young Adults in the U.S. Am J
Prev Med. 2017;53(1):1-8.
115. Nixon CL. Current perspectives: the impact of cyberbullying on
adolescent health. Adolesc Health Med Ther. 2014;5:143-158.
116. Chokshi DA. Vicious and Virtuous Cycles in Health. JAMA
Health Forum. 2023;4(2):e230505.
117. Wang J, Mann F, Lloyd-Evans B, Ma R, Johnson S. Associations
between loneliness and perceived social support and outcomes
of mental health problems: a systematic review. BMC Psychiatry.
2018;18(1):156.
118. Yu G, Sessions JG, Fu Y, Wall M. A multilevel cross-lagged
structural equation analysis for reciprocal relationship between
social capital and health. Social Science & Medicine. 2015;142:1-8.
REFERENCES
119. Saeri AK, Cruwys T, Barlow FK, Stronge S, Sibley CG. Social
connectedness improves public mental health: Investigating
bidirectional relationships in the New Zealand attitudes and
values survey. Australian & New Zealand Journal of Psychiatry.
2017;52(4):365-374.
120. Seppala E, Rossomando T, Doty J. Social Connection and
Compassion: Important Predictors of Health and Well-Being. Social
Research. 2013;80.
121. Brown KM, Hoye R, Nicholson M. Self-Esteem, Self-Efficacy,
and Social Connectedness as Mediators of the Relationship
Between Volunteering and Well-Being. Journal of Social Service
Research. 2012;38(4):468-483.
122. McClain C, Vogels E, Perrin A, Sechopoulos S, Rainie L. The
Internet and the Pandemic. Pew Research Center; 2021.
123. AmeriCorps. Volunteering and Civic Life in America Research
Summary. 2021.
124. Leigh-Hunt N, Bagguley D, Bash K, et al. An overview of
systematic reviews on the public health consequences of social
isolation and loneliness. Public Health. 2017;152:157-171.
125. Shor E, Roelfs DJ. Social contact frequency and all-cause
mortality: a meta-analysis and meta-regression. Social Science &
Medicine. 2015;128:76-86.
126. Pinquart M, Duberstein PR. Associations of social networks
with cancer mortality: a meta-analysis. Crit Rev Oncol Hematol.
2010;75(2):122-137.
127. Rico-Uribe LA, Caballero FF, Martin-Maria N, Cabello M,
Ayuso-Mateos JL, Miret M. Association of loneliness with all-cause
mortality: A meta-analysis. PLoS One. 2018;13(1):e0190033.
128. Holt-Lunstad J, Smith TB, Layton JB. Social relationships
and mortality risk: a meta-analytic review. PLoS Med.
2010;7(7):e1000316.
129. Berkman LF, Syme SL. Social networks, host resistance,
and mortality: a nine-year follow-up study of Alameda County
residents. Am J Epidemiol. 1979;109(2):186-204.
130. Pantell M, Rehkopf D, Jutte D, Syme SL, Balmes J, Adler N.
Social isolation: a predictor of mortality comparable to traditional
clinical risk factors. Am J Public Health. 2013;103(11):2056-2062.
131. Howick J, Kelly P, Kelly M. Establishing a causal link between
social relationships and health using the Bradford Hill Guidelines.
SSM Popul Health. 2019;8:100402.
132. Czajkowski SM, Arteaga SS, Burg MM. Social support and
cardiovascular disease. In: Handbook of Cardiovascular Behavioral
Medicine. Springer; 2022:605-630.
133. Cené CW, Beckie TM, Sims M, et al. Effects of Objective and
Perceived Social Isolation on Cardiovascular and Brain Health: A
Scientific Statement From the American Heart Association. Journal
of the American Heart Association. 2022;11(16):e026493.
134. Caspi A, Harrington H, Moffitt TE, Milne BJ, Poulton R. Socially
Isolated Children 20 Years Later: Risk of Cardiovascular Disease.
Archives of Pediatrics & Adolescent Medicine. 2006;160(8):805-811.

76Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
135. Danese A, Moffitt TE, Harrington H, et al. Adverse childhood
experiences and adult risk factors for age-related disease:
depression, inflammation, and clustering of metabolic risk markers.
Arch Pediatr Adolesc Med. 2009;163(12):1135-1143.
136. Manemann SM, Chamberlain AM, Roger VL, et al. Perceived
Social Isolation and Outcomes in Patients With Heart Failure. J Am
Heart Assoc. 2018;7(11).
137. Gorji MH, Fatahian A, Farsavian A. The impact of perceived
and objective social isolation on hospital readmission in patients
with heart failure: a systematic review and meta-analysis of
observational studies. General Hospital Psychiatry. 2019;60:27-36.
138. Smith RW, Barnes I, Green J, Reeves GK, Beral V, Floud S.
Social isolation and risk of heart disease and stroke: analysis
of two large UK prospective studies. Lancet Public Health.
2021;6(4):e232-e239.
139. National Center for Chronic Disease Prevention and Health
Promotion. Heart Disease and Stroke. Centers for Disease Control
and Prevention,. https://www.cdc.gov/chronicdisease/resources/
publications/factsheets/heart-disease-stroke.htm. Published 2022.
Accessed April 2023.
140. Harding BN, Hawley CN, Kalinowski J, et al. Relationship
between social support and incident hypertension in the Jackson
Heart Study: a cohort study. BMJ Open. 2022;12(3):e054812.
141. National Center for Chronic Disease Prevention and Health
Promotion, Division for Heart Disease and Stroke Prevention. High
Blood Pressure Symptoms and Causes. Centers for Disease Control
and Prevention https://www.cdc.gov/bloodpressure/about.htm.
Published 2021. Accessed April 2023.
142. Cornwell EY, Waite LJ. Social network resources and management
of hypertension. J Health Soc Behav. 2012;53(2):215-231.
143. Ueno T, Nakagomi A, Tsuji T, Kondo K. Association between
social participation and hypertension control among older
people with self-reported hypertension in Japanese communities.
Hypertension Research. 2022;45:1-6.
144. Magrin ME, D’Addario M, Greco A, et al. Social support and
adherence to treatment in hypertensive patients: a meta-analysis.
Ann Behav Med. 2015;49(3):307-318.
145. Shahin W, Kennedy GA, Stupans I. The association
between social support and medication adherence in patients
with hypertension: A systematic review. Pharm Pract (Granada).
2021;19(2):2300.
146. Pan J, Hu B, Wu L, Li Y. The Effect of Social Support on
Treatment Adherence in Hypertension in China. Patient Prefer
Adherence. 2021;15:1953-1961.
147. de Wit M, Trief PM, Huber JW, Willaing I. State of the art:
understanding and integration of the social context in diabetes
care. Diabet Med. 2020;37(3):473-482.
148. Brinkhues S, Dukers-Muijrers N, Hoebe C, et al. Socially
isolated individuals are more prone to have newly diagnosed and
prevalent type 2 diabetes mellitus - the Maastricht study. BMC
Public Health. 2017;17(1):955.
REFERENCES
149. Brinkhues S, Dukers-Muijrers N, Hoebe C, et al. Social
Network Characteristics Are Associated With Type 2
Diabetes Complications: The Maastricht Study. Diabetes Care.
2018;41(8):1654-1662.
150. Altevers J, Lukaschek K, Baumert J, et al. Poor structural
social support is associated with an increased risk of Type 2
diabetes mellitus: findings from the MONICA/KORA Augsburg
cohort study. Diabet Med. 2016;33(1):47-54.
151. Meisinger C, Kandler U, Ladwig KH. Living alone is associated
with an increased risk of type 2 diabetes mellitus in men but not
women from the general population: the MONICA/KORA Augsburg
Cohort Study. Psychosom Med. 2009;71(7):784-788.
152. Norberg M, Stenlund H, Lindahl B, Andersson C, Eriksson JW,
Weinehall L. Work stress and low emotional support is associated
with increased risk of future type 2 diabetes in women. Diabetes
Res Clin Pract. 2007;76(3):368-377.
153. Strodl E, Kenardy J. Psychosocial and non-psychosocial
risk factors for the new diagnosis of diabetes in elderly women.
Diabetes Res Clin Pract. 2006;74(1):57-65.
154. Lidfeldt J, Nerbrand C, Samsioe G, Agardh CD. Women
living alone have an increased risk to develop diabetes,
which is explained mainly by lifestyle factors. Diabetes Care.
2005;28(10):2531-2536.
155. Kelly CS, Berg CA. Close relationships and diabetes
management across the lifespan: The good, the bad, and autonomy.
Journal of Health Psychology. 2018;26(2):226-237.
156. Wiebe DJ, Helgeson V, Berg CA. The social context
of managing diabetes across the life span. Am Psychol.
2016;71(7):526-538.
157. Umeh K. Self-rated health and multimorbidity in patients with
type 2 diabetes. J Health Psychol. 2022;27(7):1659-1678.
158. Song Y, Nam S, Park S, Shin IS, Ku BJ. The Impact of Social
Support on Self-care of Patients With Diabetes: What Is the Effect
of Diabetes Type? Systematic Review and Meta-analysis. Diabetes
Educ. 2017;43(4):396-412.
159. Loprinzi PD, Ford MA. Effects of Social Support Network Size
on Mortality Risk: Considerations by Diabetes Status. Diabetes
Spectr. 2018;31(2):189-192.
160. LeRoy AS, Murdock KW, Jaremka LM, Loya A, Fagundes CP.
Loneliness predicts self-reported cold symptoms after a viral
challenge. Health Psychol. 2017;36(5):512-520.
161. Cohen S, Doyle WJ, Skoner DP, Rabin BS, Gwaltney JM,
Jr. Social ties and susceptibility to the common cold. JAMA.
1997;277(24):1940-1944.
162. Stephen G, Siobhán H, Muldoon OT, Whittaker AC. Social
cohesion and loneliness are associated with the antibody response
to COVID-19 vaccination. Brain Behav Immun. 2022;103:179-185.
163. Akhter-Khan SC, Tao Q, Ang TFA, et al. Associations of loneliness
with risk of Alzheimer’s disease dementia in the Framingham Heart
Study. Alzheimer’s & Dementia. 2021;17(10):1619-1627.
164. Donovan NJ, Wu Q, Rentz DM, Sperling RA, Marshall GA,
Glymour MM. Loneliness, depression and cognitive function in
older U.S. adults. Int J Geriatr Psychiatry. 2017;32(5):564-573.

77Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
165. Duffner LA, Deckers K, Cadar D, Steptoe A, de Vugt M, Köhler
S. The role of cognitive and social leisure activities in dementia
risk: assessing longitudinal associations of modifiable and non-
modifiable risk factors. Epidemiol Psychiatr Sci. 2022;31:e5.
166. Domènech-Abella J, Mundó J, Haro JM, Rubio-Valera M.
Anxiety, depression, loneliness and social network in the elderly:
Longitudinal associations from The Irish Longitudinal Study on
Ageing (TILDA). J Affect Disord. 2019;246:82-88.
167. Loades ME, Chatburn E, Higson-Sweeney N, et al. Rapid
Systematic Review: The Impact of Social Isolation and Loneliness
on the Mental Health of Children and Adolescents in the Context
of COVID-19. Journal of the American Academy of Child & Adolescent
Psychiatry. 2020;59(11):1218-1239.e1213.
168. Choi KW, Stein MB, Nishimi KM, et al. An Exposure-Wide and
Mendelian Randomization Approach to Identifying Modifiable
Factors for the Prevention of Depression. Am J Psychiatry.
2020;177(10):944-954.
169. Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby
EA, Joiner TE, Jr. The interpersonal theory of suicide. Psychol Rev.
2010;117(2):575-600.
170. Shaw RJ, Cullen B, Graham N, et al. Living alone, loneliness
and lack of emotional support as predictors of suicide and self-
harm: A nine-year follow up of the UK Biobank cohort. J Affect
Disord. 2021;279:316-323.
171. Mezuk B, Rock A, Lohman MC, Choi M. Suicide risk in long‐
term care facilities: A systematic review. International journal of
geriatric psychiatry. 2014;29(12):1198-1211.
172. Du L, Shi HY, Qian Y, et al. Association between social support
and suicidal ideation in patients with cancer: A systematic review
and meta-analysis. Eur J Cancer Care (Engl). 2021;30(2):e13382.
173. Conwell Y, Van Orden K, Caine ED. Suicide in older adults.
Psychiatr Clin North Am. 2011;34(2):451-468, ix.
174. King CA, Merchant CR. Social and interpersonal factors
relating to adolescent suicidality: a review of the literature. Arch
Suicide Res. 2008;12(3):181-196.
175. Troya MI, Babatunde O, Polidano K, et al. Self-harm in older
adults: systematic review. Br J Psychiatry. 2019;214(4):186-200.
176. Brown EG, Gallagher S, Creaven A-M. Loneliness and acute
stress reactivity: A systematic review of psychophysiological
studies. Psychophysiology. 2018;55(5):e13031.
177. Leschak CJ, Eisenberger NI. Two Distinct Immune Pathways
Linking Social Relationships With Health: Inflammatory and
Antiviral Processes. Psychosom Med. 2019;81(8):711-719.
178. DiMatteo MR. Social Support and Patient Adherence
to Medical Treatment: A Meta-Analysis. Health Psychology.
2004;23:207-218.
179. Shankar A, McMunn A, Banks J, Steptoe A. Loneliness, social
isolation, and behavioral and biological health indicators in older
adults. Health Psychology. 2011;30:377-385.
180. Hooker SA, Masters KS, Park CL. A Meaningful Life is a
Healthy Life: A Conceptual Model Linking Meaning and Meaning
Salience to Health. Review of General Psychology. 2018;22(1):11-24.
REFERENCES
181. Cacioppo JT, Cacioppo S, Capitanio JP, Cole SW. The
neuroendocrinology of social isolation. Annu Rev Psychol.
2015;66:733-767.
182. Mattos Dos Santos R. Isolation, social stress, low
socioeconomic status and its relationship to immune response
in Covid-19 pandemic context. Brain Behav Immun Health.
2020;7:100103.
183. Muscatell KA. Social psychoneuroimmunology: Understanding
bidirectional links between social experiences and the immune
system. Brain Behav Immun. 2021;93:1-3.
184. Robles TF. Annual Research Review: Social relationships and
the immune system during development. J Child Psychol Psychiatry.
2021;62(5):539-559.
185. Donovan M, Mackey CS, Platt GN, et al. Social isolation
alters behavior, the gut-immune-brain axis, and neurochemical
circuits in male and female prairie voles. Neurobiology of Stress.
2020;13:100278.
186. Dill-McFarland KA, Tang Z-Z, Kemis JH, et al. Close social
relationships correlate with human gut microbiota composition.
Scientific Reports. 2019;9(1):703.
187. Guidi J, Lucente M, Sonino N, Fava GA. Allostatic Load and Its
Impact on Health: A Systematic Review. Psychother Psychosom.
2021;90(1):11-27.
188. Furman D, Campisi J, Verdin E, et al. Chronic inflammation
in the etiology of disease across the life span. Nat Med.
2019;25(12):1822-1832.
189. Yang YC, Schorpp K, Harris KM. Social support, social strain
and inflammation: evidence from a national longitudinal study of
U.S. adults. Soc Sci Med. 2014;107:124-135.
190. McHugh Power J, Carney S, Hannigan C, et al. Systemic
inflammatory markers and sources of social support among older
adults in the Memory Research Unit cohort. J Health Psychol.
2019;24(3):397-406.
191. Ershler WB, Keller ET. Age-associated increased interleukin-6
gene expression, late-life diseases, and frailty. Annu Rev Med.
2000;51:245-270.
192. Fortmann AL, Gallo LC. Social support and nocturnal
blood pressure dipping: a systematic review. Am J Hypertens.
2013;26(3):302-310.
193. Teoh AN, Hilmert C. Social support as a comfort or an
encouragement: A systematic review on the contrasting effects
of social support on cardiovascular reactivity. Br J Health Psychol.
2018;23(4):1040-1065.
194. Li H, Xia N. The role of oxidative stress in cardiovascular
disease caused by social isolation and loneliness. Redox Biol.
2020;37:101585.
195. Froemke RC, Young LJ. Oxytocin, Neural Plasticity, and Social
Behavior. Annual Review of Neuroscience. 2021;44(1):359-381.
196. Hostinar CE. Recent Developments in the Study of Social
Relationships, Stress Responses, and Physical Health. Curr Opin
Psychol. 2015;5:90-95.

78Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
197. Scatliffe N, Casavant S, Vittner D, Cong X. Oxytocin and early
parent-infant interactions: A systematic review. Int J Nurs Sci.
2019;6(4):445-453.
198. Silver L, Van Kessel P, Huang C, Clancy L, Gubbala S. What
Makes Life Meaningful? Views From 17 Advanced Economies. Pew
Research Center; 2021.
199. Petrova D, Garcia-Retamero R, Catena A. Lonely hearts
don’t get checked: On the role of social support in screening for
cardiovascular risk. Preventive Medicine. 2015;81:202-208.
200. Kim ES, Strecher VJ, Ryff CD. Purpose in life and use
of preventive health care services. Proc Natl Acad Sci U S A.
2014;111(46):16331-16336.
201. Southwick SM, Sippel L, Krystal J, Charney D, Mayes L,
Pietrzak R. Why are some individuals more resilient than others: the
role of social support. World Psychiatry. 2016;15(1):77-79.
202. Kivimäki M, Steptoe A. Effects of stress on the development
and progression of cardiovascular disease. Nature Reviews
Cardiology. 2018;15(4):215-229.
203. Schore AN. The effects of early relational trauma on right
brain development, affect regulation, and infant mental health.
Infant Mental Health Journal. 2001;22(1-2):201-269.
204. Chandola T, Brunner E, Marmot M. Chronic stress at
work and the metabolic syndrome: prospective study. BMJ.
2006;332(7540):521-525.
205. McEwen BS. Neurobiological and Systemic Effects of Chronic
Stress. Chronic Stress. 2017;1:2470547017692328.
206. Birmingham WC, Holt-Lunstad J. Social aggravation:
Understanding the complex role of social relationships on stress
and health-relevant physiology. Int J Psychophysiol. 2018;131:13-23.
207. Kent de Grey RG, Uchino BN, Trettevik R, Cronan S, Hogan
JN. Social support and sleep: A meta-analysis. Health Psychol.
2018;37(8):787-798.
208. Kobayashi LC, Steptoe A. Social Isolation, Loneliness, and
Health Behaviors at Older Ages: Longitudinal Cohort Study. Ann
Behav Med. 2018;52(7):582-593.
209. Schrempft S, Jackowska M, Hamer M, Steptoe A. Associations
between social isolation, loneliness, and objective physical activity
in older men and women. BMC Public Health. 2019;19(1):74.
210. Christakis NA, Fowler JH. Social contagion theory: examining
dynamic social networks and human behavior. Stat Med.
2013;32(4):556-577.
211. Driscoll SD. Barriers and facilitators to cervical cancer
screening in high incidence populations: A synthesis of qualitative
evidence. Women Health. 2016;56(4):448-467.
212. Miller TA, Dimatteo MR. Importance of family/social support
and impact on adherence to diabetic therapy. Diabetes Metab Syndr
Obes. 2013;6:421-426.
213. Mendonça G, Cheng LA, Mélo EN, de Farias Júnior JC. Physical
activity and social support in adolescents: a systematic review.
Health Educ Res. 2014;29(5):822-839.
REFERENCES
214. Macdonald-Wallis K, Jago R, Sterne JAC. Social Network
Analysis of Childhood and Youth Physical Activity: A Systematic
Review. American Journal of Preventive Medicine. 2012;43(6):636-642.
215. Christakis NA, Fowler JH. The Collective Dynamics of Smoking
in a Large Social Network. New England Journal of Medicine.
2008;358(21):2249-2258.
216. Moore S, Teixeira A, Stewart S. Effect of network social capital
on the chances of smoking relapse: a two-year follow-up study of
urban-dwelling adults. Am J Public Health. 2014;104(12):e72-76.
217. Blok DJ, de Vlas SJ, van Empelen P, van Lenthe FJ. The role
of smoking in social networks on smoking cessation and relapse
among adults: A longitudinal study. Prev Med. 2017;99:105-110.
218. DuBois DL, Portillo N, Rhodes JE, Silverthorn N, Valentine JC.
How Effective Are Mentoring Programs for Youth? A Systematic
Assessment of the Evidence. Psychological Science in the Public
Interest. 2011;12(2):57-91.
219. Steiner RJ, Sheremenko G, Lesesne C, Dittus PJ, Sieving RE,
Ethier KA. Adolescent Connectedness and Adult Health Outcomes.
Pediatrics. 2019;144(1).
220. Beal DJ, Cohen RR, Burke MJ, McLendon CL. Cohesion and
Performance in Groups: A Meta-Analytic Clarification of Construct
Relations. Journal of Applied Psychology. 2003;88:989-1004.
221. Tu M, Cheng Z, Liu W. Spotlight on the Effect of Workplace
Ostracism on Creativity: A Social Cognitive Perspective. Frontiers in
Psychology. 2019;10.
222. Kwan HK, Zhang X, Liu J, Lee C. Workplace Ostracism and
Employee Creativity: An Integrative Approach Incorporating
Pragmatic and Engagement Roles. Journal of Applied Psychology.
2018;103:1358–1366.
223. Patel A., Plowman S. The Increasing Importance of a Best
Friend at Work. In. Workplace: Gallup Inc.,; 2022.
224. Mann A. Why We Need Best Friends at Work. Gallup, Inc.; 2018.
225. Velando-Soriano A, Ortega-Campos E, Gómez-Urquiza
JL, Ramírez-Baena L, De La Fuente EI, Cañadas-De La Fuente
GA. Impact of social support in preventing burnout syndrome in
nurses: A systematic review. Japan Journal of Nursing Science.
2020;17(1):e12269.
226. White C, Green RA, Ferguson S, et al. The influence of social
support and social integration factors on return to work outcomes
for individuals with work-related injuries: a systematic review.
Journal of occupational rehabilitation. 2019;29(3):636-659.
227. Chetty R, Jackson MO, Kuchler T, et al. Social capital I:
measurement and associations with economic mobility. Nature.
2022;608(7921):108-121.
228. Chetty R, Jackson MO, Kuchler T, et al. Social capital
II: determinants of economic connectedness. Nature.
2022;608(7921):122-134.
229. Wilson J. Volunteering. Annual review of sociology. 2000:215-
240.
230. Jastrzab J, Giordono L, Chase A, et al. Serving Country and
Community: A Longitudinal Study of Service in AmeriCorps. Washington,
DC: Corporation for National and Community Service; 2004.

79Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
231. Spera C, Ghertner R, Nerino A, DiTommaso A. Out of work?
Volunteers Have Higher Odds of Getting Back to Work. Nonprofit
and Voluntary Sector Quarterly. 2015;44(5):886-907.
232. National Academies of Sciences Engineering and Medicine
(NASEM). Enhancing Community Resilience through Social Capital
and Connectedness: Stronger Together! Washington, DC: The
National Academies Press; 2021.
233. Agency for Toxic Substances and Disease Registry. Concepts
of Community. U.S. Department of Health and Human Services,.
https://www.atsdr.cdc.gov/communityengagement/pce_concepts.
html. Published 2015. Accessed April 2023.
234. Abbott S, Freeth D. Social capital and health: starting to
make sense of the role of generalized trust and reciprocity. J Health
Psychol. 2008;13(7):874-883.
235. Putnam RD. Better Together: Report of the Saguaro Seminar on
Civic Engagement in America. 2000.
236. Fu F, Nowak MA, Christakis NA, Fowler JH. The Evolution of
Homophily. Scientific Reports. 2012;2(1):845.
237. Szreter S, Woolcock M. Health by association? Social capital,
social theory, and the political economy of public health. Int J
Epidemiol. 2004;33(4):650-667.
238. Poortinga W. Community resilience and health: The role of
bonding, bridging, and linking aspects of social capital. Health &
Place. 2012;18(2):286-295.
239. Assistant Secretary for Planning and Evaluation. How Human
Services Programs Can Use Social Capital to Improve Participant
Well-Being and Economic Mobility. U.S. Department of Health and
Human Services. https://aspe.hhs.gov/topics/human-services/
how-human-services-programs-can-use-social-capital-improve-
participant-well-being-economic-mobility. Published n.d. Accessed
April 2023.
240. Hunt V, Layton, D., Prince, S.,. Why diversity matters.
McKinsey&Company; 2015.
241. Hyyppä M. Healthy ties: Social capital, population health and
survival. 2010.
242. Villalonga-Olives E, Wind T, Kawachi I. Social capital
interventions in public health: A systematic review. Social Science &
Medicine. 2018;212:203-218.
243. Gilbert KL, Quinn SC, Goodman RM, Butler J, Wallace J. A
meta-analysis of social capital and health: A case for needed
research. Journal of Health Psychology. 2013;18(11):1385-1399.
244. Office of Disease Prevention and Health Promotion, Office of
the Assistant Secretary for Health. Healthy People 2030. Office
of the Secretary, U.S. Department of Health and Human Services.
https://health.gov/healthypeople/objectives-and-data/browse-
objectives/social-and-community-context. Published n.d. Accessed
April 2023.
245. My Health My Community. Social Connection and Health. 2018.
246. Nieminen T, Harkanen T, Martelin T, Borodulin K, Koskinen
S. Social capital and all-cause mortality among Finnish men and
women aged 30-79. Eur J Public Health. 2015;25(6):972-978.
REFERENCES
247. Zoorob MJ, Salemi JL. Bowling alone, dying together: The role
of social capital in mitigating the drug overdose epidemic in the
United States. Drug Alcohol Depend. 2017;173:1-9.
248. Kawachi I, Kennedy BP, Lochner K, Prothrow-Stith D. Social
capital, income inequality, and mortality. Am J Public Health.
1997;87(9):1491-1498.
249. Brewster A, Lee S, Curry L, Bradley E. Association Between
Community Social Capital and Hospital Readmission Rates.
Population Health Management. 2019;22(1):40-47.
250. Takada S, Gorbach P, Brookmeyer R, Shoptaw S. Associations
of social capital resources and experiences of homophobia with HIV
transmission risk behavior and HIV care continuum among men who
have sex with men in Los Angeles. AIDS Care. 2021;33(5):663-674.
251. Anderson B. HIV Stigma and Discrimination Persist, Even in
Health Care. Virtual Mentor. 2009;11(12):998-1001.
252. Nugraheni R, Murti B, Irawanto ME, Sulaiman ES,
Pamungkasari EP. The social capital effect on HIV/AIDS preventive
efforts: a meta-analysis. J Med Life. 2022;15(10):1212-1217.
253. Ransome Y, Thurber KA, Swen M, Crawford ND, German
D, Dean LT. Social capital and HIV/AIDS in the United States:
Knowledge, gaps, and future directions. SSM - Population Health.
2018;5:73-85.
254. Jung M, Lin L, Viswanath K. Associations between health
communication behaviors, neighborhood social capital, vaccine
knowledge, and parents’ H1N1 vaccination of their children. Vaccine.
2013;31(42):4860-4866.
255. Rönnerstrand B. Social capital and immunization against
the 2009 A(H1N1) pandemic in the American States. Public Health.
2014;128(8):709-715.
256. Rönnerstrand B. Contextual generalized trust and immunization
against the 2009 A(H1N1) pandemic in the American states: A
multilevel approach. SSM - Population Health. 2016;2:632-639.
257. Ferwana I, Varshney LR. Social capital dimensions are
differentially associated with COVID-19 vaccinations, masks, and
physical distancing. PLoS One. 2021;16(12):e0260818.
258. Hasan MZ, Dean LT, Kennedy CE, Ahuja A, Rao KD, Gupta
S. Social capital and utilization of immunization service: A
multilevel analysis in rural Uttar Pradesh, India. SSM Popul Health.
2020;10:100545.
259. Cronin CE, Franz B, Garlington S. Population health
partnerships and social capital: Facilitating hospital-community
partnerships. SSM Popul Health. 2021;13:100739.
260. Saint Onge JM, Brooks JV. The exchange and use of cultural
and social capital among community health workers in the United
States. Sociology of Health & Illness. 2021;43(2):299-315.
261. Bartscher AK, Seitz S, Siegloch S, Slotwinski M, Wehrhöfer N.
Social capital and the spread of Covid-19: Insights from European
countries. Journal of Health Economics. 2021;80:102531.
262. Borgonovi F, Andrieu E. Bowling together by bowling
alone: Social capital and Covid-19. Social science & medicine.
2020;265:113501.

80Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
263. Fraser T, Aldrich DP, Page-Tan C. Bowling alone or distancing
together? The role of social capital in excess death rates from
COVID19. Soc Sci Med. 2021;284:114241.
264. Fraser T, Page-Tan C, Aldrich DP. Social capital’s impact
on COVID-19 outcomes at local levels. Scientific Reports.
2022;12(1):6566.
265. Makridis CA, Wu C. How social capital helps communities
weather the COVID-19 pandemic. PloS one. 2021;16(1):e0245135.
266. COVID-19 National Preparedness Collaborators. Pandemic
preparedness and COVID-19: an exploratory analysis of infection
and fatality rates, and contextual factors associated with
preparedness in 177 countries, from Jan 1, 2020, to Sept 30, 2021.
Lancet. 2022;399(10334):1489-1512.
267. Equitable Long-Term Recovery and Resilience Interagency
Workgroup. Federal Plan for Equitable Long-Term Recovery
and Resilience for Social, Behavioral, and Community Health.
Washington, D.C.: U.S. Department of Health and Human Services,
Office of the Assistant Secretary for Health, U Office of Disease
Prevention and Health Promotion; 2022.
268. National Institutes of Standards and Technology. Community
Resilience. U.S. Department of Commerce. https://www.nist.gov/
community-resilience. Published n.d. Accessed April 2023.
269. Office of the Assistant Secretary for Preparedness and
Response. Community Resilience. U.S. Department of Health and
Human Services. https://www.phe.gov/Preparedness/planning/
abc/Pages/community-resilience.aspx. Published 2015. Accessed
April 2023.
270. Losee JE, Webster GD, McCarty C. Social network connections
and increased preparation intentions for a disaster. Journal of
Environmental Psychology. 2022;79:101726.
271. Stuart BA, Taylor EJ. The Effect of Social Connectedness on
Crime: Evidence from the Great Migration. The Review of Economics
and Statistics. 2021;103(1):18-33.
272. Ross CE, Jang SJ. Neighborhood disorder, fear, and mistrust:
The buffering role of social ties with neighbors. American journal of
community psychology. 2000;28(4):401-420.
273. Resnick MD, Ireland M, Borowsky I. Youth violence
perpetration: what protects? What predicts? Findings from the
National Longitudinal Study of Adolescent Health. J Adolesc Health.
2004;35(5):424.e421-410.
274. David-Ferdon C, Vivolo-Kantor AM, Dahlberg LL, Marshall KJ,
Rainford N, Hall JE. A comprehensive technical package for the
prevention of youth violence and associated risk behaviors. 2016.
275. Riley C, Roy B, Harari N, et al. Preparing for Disaster: a Cross-
Sectional Study of Social Connection and Gun Violence. J Urban
Health. 2017;94(5):619-628.
276. Lanfear CC. Collective efficacy and the built environment.
Criminology. 2022;60(2):370-396.
277. Lederman, Daniel, Norman Loayza, and Ana Maria Menendez.
“Violent crime: does social capital matter?.” Economic Development
and Cultural Change 50.3 (2002): 509-539.
REFERENCES
278. Milam AJ, Buggs SA, Furr-Holden CD, Leaf PJ, Bradshaw
CP, Webster D. Changes in Attitudes toward Guns and Shootings
following Implementation of the Baltimore Safe Streets
Intervention. J Urban Health. 2016;93(4):609-626.
279. Butts JA, Roman CG, Bostwick L, Porter JR. Cure Violence:
A Public Health Model to Reduce Gun Violence. Annual Review of
Public Health. 2015;36(1):39-53.
280. National Conference on Citizenship (NCOC). Civic Health and
Unemployment: Can Engagement Strengthen the Economy? 2011.
281. Knight Foundation. Got Love For Your Community? It
M
ay C
reate Economic Growth, Gallup Study Says. https://
knightfoundation.org/press/releases/got-love-for-your-community-
it-may-create-economic/. Published 2010. Accessed April 2023.
282. Zenou Y. Social Interactions and Labor Market Outcomes in
Cities Bonn, Germany: The Institute for the Study of Labor; 2008.
IFN Working Paper No. 755,.
283. Ballard PJ, Hoyt LT, Pachucki MC. Impacts of Adolescent
and Young Adult Civic Engagement on Health and Socioeconomic
Status in Adulthood. Child Development. 2019;90(4):1138-1154.
284. Warner M. Building Social Capital: The Role of Local
Government. The Journal of Socio-Economics. 2001;30:187-192.
285. Department for Digital, Culture, Media and Sport. A connected
society: A Strategy for tackling loneliness – laying the foundations
for change. London, UK: HM Government; 2018.
286. Duke, N. N., Skay, C. L., Pettingell, S. L., & Borowsky, I. W.
(2009). From Adolescent Connections to Social Capital: Predictors
of Civic Engagement in Young Adulthood. Journal of Adolescent
Health, 44(2), 161-168.
287. Campbell DE. Social Networks and Political Participation.
Annual Review of Political Science. 2013;16(1):33-48.
288. Kim Y. Toward an effective government–public relationship:
Organization–public relationship based on a synthetic approach to
public segmentation. Public Relations Review. 2015;41(4):456-460.
289. Ledingham JA. Government-community relationships:
extending the relational theory of public relations. Public Relations
Review. 2001;27:285-295.
290. Everett JA, Faber NS, Crockett M. Preferences and beliefs in
ingroup favoritism. Front Behav Neurosci. 2015;9:15.
291. Merton RK. Insiders and Outsiders: A Chapter in the Sociology
of Knowledge. American Journal of Sociology. 1972;78(1):9-47.
292. Villalonga-Olives E, Kawachi I. The dark side of social capital:
A systematic review of the negative health effects of social capital.
Soc Sci Med. 2017;194:105-127.
293. Mccoy J, Press B, Somer M, Tuncel O. Reducing Pernicious
Polarization: A Comparative Historical Analysis of Depolarization
Carnegie Endowment for International Peace; 2022.
294. Kalmoe N, Mason L. Lethal mass partisanship: Prevalence,
correlates, & electoral contingencies. National Capital Area
Political Science Association American Politics Meeting; 2019.
295. Hampton K, Sessions L, Ja Her E, Rainie L. Social isolation and
new technology. Pew Research Center; 2009.

81Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
REFERENCES
296. Mutz DC. Cross-Cutting Social Networks: Testing Democratic
Theory in Practice. The American Political Science Review.
2002;96(1):111-126.
297. McPherson M, Smith-Lovin L, Brashears ME. Social Isolation in
America: Changes in Core Discussion Networks over Two Decades.
American Sociological Review. 2006;71(3):353-375.
298. Lee B, Bearman P. Political isolation in America. Network
Science. 2020;8(3):333-355.
299. Green T. Republicans and Democrats alike say it’s stressful
t
o t
alk politics with people who disagree. 2021. https://www.
pewresearch.org/fact-tank/2021/11/23/republicans-and-
democrats-alike-say-its-stressful-to-talk-politics-with-people-
who-disagree/.
300. Pew Research Center, Edelman. Edelman Trust Barometer
Global Report 2022.
301. Hurlburt H, Argo Ben Itzhak N, Brown R, Livingston L, Owens
S. Building U.S. Resilience to Political Violence: A Globally Informed
Framework for Analysis and Action. New America; 2019.
302. World Health Organization. Social Isolation and Loneliness. World
Health Organization. https://www.who.int/teams/social-determinants-
of-health/demographic-change-and-healthy-ageing/social-isolation-
and-loneliness. Published 2023. Accessed April 2023.
303. Healthy Places by Design, Social Isolation Learning Network.
Socially Connected Communities: Solutions for Social Isolation.
Healthy Places by Design; 2021.
304. Smith TB, Workman C, Andrews C, et al. Effects of
psychosocial support interventions on survival in inpatient and
outpatient healthcare settings: A meta-analysis of 106 randomized
controlled trials. PLoS Med. 2021;18(5):e1003595.
305. Holt-Lunstad J, Perissinotto C. Social Isolation and
Loneliness as Medical Issues. New England Journal of Medicine.
2023;388(3):193-195.
306. National Academies of Sciences Engineering and Medicine
(NASEM). Toward a 21st Century National Data Infrastructure:
Mobilizing Information for the Common Good. Washington, DC: The
National Academies Press; 2023.
307. Holt-Lunstad J. National Health Guidelines for Social
Connection: What Is the Evidence in Support and What Might
the Guidelines Say? Policy Insights from the Behavioral and Brain
Sciences,. 2023;10:41-50.
308. National Academy of Medicine. National Plan for Health
Workforce Well-Being. Washington, DC: The National Academies
Press; 2022.
309. United States Department of Health and Human Services.
Addressing Health Worker Burnout: The U.S. Surgeon General’s
Advisory on Building a Thriving Health Workforce. Washington, D.C.:
U.S. Department of Health and Human Services, Office of the U.S.
Surgeon General; 2022.
310. Division of Population Health, National Center for Chronic
Disease Prevention and Health Promotion. Whole School, Whole
Community, Whole Child (WSCC). Centers for Disease Control and
Prevention,. https://www.cdc.gov/healthyschools/wscc/index.htm.
Published 2023. Accessed April 2023.
311. Roseth CJ, Johnson DW, Johnson RT. Promoting early
adolescents’ achievement and peer relationships: the effects
of cooperative, competitive, and individualistic goal structures.
Psychol Bull. 2008;134(2):223-246.
312. Mental Health America. Is Your Child Lonely? (For Parents).
Mental Health America. https://mhanational.org/your-child-lonely-
parents. Published 2023. Accessed April 2023.
313. Ehmke R, Allerhand L, Vibert B. How to Help Kids Who Are
Lonely. Child Mind Institute https://childmind.org/article/how-to-
help-kids-who-are-lonely/. Published 2022. Accessed April 2023.
314. Canevello A, Crocker J. Creating good relationships:
responsiveness, relationship quality, and interpersonal goals. J Pers
Soc Psychol. 2010;99(1):78-106.
315. Caputo A. The Relationship Between Gratitude and Loneliness:
The Potential Benefits of Gratitude for Promoting Social Bonds. Eur
J Psychol. 2015;11(2):323-334.
316. Substance Abuse and Mental Health Services Administration.
988 Suicide and Crisis Lifeline. Substance Abuse and Mental
Health Services Administration,. https://988lifeline.org/. Published
n.d. Accessed April 2023.
317. Roelfs DJ, Shor E, Curreli M, Clemow L, Burg MM, Schwartz JE.
Widowhood and mortality: a meta-analysis and meta-regression.
Demography. 2012;49(2):575-606.
318. Roelfs DJ, Shor E, Kalish R, Yogev T. The rising relative risk
of mortality for singles: meta-analysis and meta-regression. Am J
Epidemiol. 2011;174(4):379-389.
319. Fedak KM, Bernal A, Capshaw ZA, Gross S. Applying the
Bradford Hill criteria in the 21st century: how data integration has
changed causal inference in molecular epidemiology. Emerging
Themes in Epidemiology. 2015;12(1):14.
320. Cox LA, Jr. Modernizing the Bradford Hill criteria for assessing
causal relationships in observational data. Crit Rev Toxicol.
2018;48(8):682-712.
321. Peng A, Tang Y, He S, Ji S, Dong B, Chen L. Association
between loneliness, sleep behavior and quality: a propensity-
score-matched case-control study. Sleep Med. 2021;86:19-24.
322. Elovainio M, Hakulinen C, Pulkki-Råback L, et al. Contribution
of risk factors to excess mortality in isolated and lonely individuals:
an analysis of data from the UK Biobank cohort study. Lancet Public
Health. 2017;2(6):e260-e266.
323. Zheng C, He MH, Huang JR, He Y. Causal Relationships
Between Social Isolation and Osteoarthritis: A Mendelian
Randomization Study in European Population. Int J Gen Med.
2021;14:6777-6786.
324. Cacioppo JT, Cacioppo S, Cole SW, Capitanio JP, Goossens
L, Boomsma DI. Loneliness across phylogeny and a call for
comparative studies and animal models. Perspect Psychol Sci.
2015;10(2):202-212.
325. Cole SW, Capitanio JP, Chun K, Arevalo JM, Ma J, Cacioppo
JT. Myeloid differentiation architecture of leukocyte transcriptome
dynamics in perceived social isolation. Proc Natl Acad Sci U S A.
2015;112(49):15142-15147.

82Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community
